Abstract
Anterior open bite can be defined as a malocclusion with a negative vertical discrepancy between the incisal edges of the upper and lower anterior teeth, which do not have occlusal contacts with the antagonists and sometimes extends to the canines and, less frequently, to the premolars is one of the malocclusions with the greatest aesthetic and/or functional impairment. Anterior open bite can have several etiologies: finger sucking and/or pacifier, oral breathing, onychophagia, lip interposition, atypical swallowing, tongue interposition when uttering phonemes and anterior posture of the tongue at rest. Orofacial myofunctional disorders are present in cases of anterior open bite, generally associated with etiologies and adapt to this altered morphological condition. Regarding the anterior opening amplitude, the anterior open bite is classified as: minimum up to 1 mm, moderate between 1 and 5 mm and severe +5 mm [1]. Open bite can be classified into: maxillary, mandibular and hybrid open bite [2]. Myofunctional therapy is considered a treatment method that can increase muscle strength, cause changes in functional patterns and thus prevent deviations in craniofacial development, as it promotes new posture of structures at rest and during the performance of the functions of the stomatognathic system [3]. The hyperboloid is an instrument for increasing muscle tone and when used in chewing, it is efficient in inducing growth and remodeling. The hyperboloid fills a gap in the modern diet, with the consistency of hard, raw and dry foods [4]. Exercises with a size M hyperboloid with wire were prescribed as an initial approach. After 2 months of treatment, there was an improvement in the interincisor distance. The exercise was maintained for another 5 months. He stopped attending appointments for 2 years and 2 months. Upon his return, the results of the functional examination of swallowing, chewing, protrusion and laterality were observed, and we opted for the installation of the SN3. the hyperboloid, in this case, showed its efficiency in balancing the stomatognathic system.
1. Introduction
Humans use their mouths for different functions: The first functions of the mouth are: swallowing and sucking, which occur during intrauterine life, innate functions that remain until the end of life. Chewing and speaking are learned functions. It is necessary for the individual to be subjected to adequate stimuli so that they develop the ability to chew and speak [5]. Breathing, sucking, chewing and swallowing are vital functions for humans and are called vegetative reflex functions. Vegetative reflex functions are considered pre-linguistic because they prepare the phonoarticulatory organs, adapting them for speech production [5]. If we have a balance between functions, we will have correct craniofacial growth and development.
Muscle hypotonia is largely responsible for growth disorders. These changes are directly linked to inefficient muscle work. Teeth and alveolar bones are exposed to antagonistic forces and pressures arising mainly from muscular function, which in part can determine tooth position. On the other hand, the intrinsic forces of the lips and tongue at rest generate a condition of balance for the position of the teeth. Equilibrium exists when a body at rest is subjected to forces in several directions, but does not undergo acceleration or, in the case of teeth, does not undergo displacement [5].
The receptors – proprioceptors and exteroreceptors, are capable of capturing mechanical stimuli and informing the central nervous system (CNS). The tongue and oral mucosa have sensory receptors, the density in both locations is not homogeneous. The tip of the tongue has an infinitely greater density of receptors in its anterior part than in the rest. The mouth's ability to discriminate a sensory stimulus is very large, therefore, small stimuli can generate many afferents – inputs to the central nervous system (CNS) [6].
Exercise generates stimuli in the largest number of sensory receptors, afferents – inputs. This set of inputs generated in the receptors of the oral mucosa and tongue will be computed in the CNS and orders – efferences – outputs, will be sent to the periphery, reaching the effector organs, muscles, tendons, ligaments and fascia [6]. Myofunctional therapy is considered a treatment method that can increase muscle strength, cause changes in functional patterns, and thus prevent deviations in craniofacial development, as it promotes new posture of structures at rest and during the performance of the functions of the stomatognathic system [3].
Neuroclusal Rehabilitation (NOR) was already thinking about this deficit that modern nutrition brought to craniofacial growth and development. Neuroclusal rehabilitation (NOR), based on Claude Bernard’s principle that “function creates the organ, and the organ provides the function”. The function starts from a neural excitation, if this is physiological it will produce a physiological function and development and if on the contrary it is pathological, the developmental response will be equally pathological. Civilized nutrition does not excite function, if there is no function, there will be no development of the organ [7].
The effects of mechanical stimulation on connective tissues, especially bone tissue, are considered beneficial. The periodicity, magnitude or frequency of the applied stimulus characterizes the cellular response [8].
There are three different ways of applying a mechanical load to a bone substrate: compression, traction and torsion. For each of these ways there will be a type of cell reaction, with expression of different genes that will generate bone remodeling and the establishment of shape. Whatever the method of mechanical stimulation perceived by bone cells, the effect generated will be propagated through the cellular connection network, which is the interconnection of osteoprogenitor cells, osteoblasts and osteocytes. Bone remodeling will occur not only at the site of the stimulus, but throughout the entire extent of this network [9].
2. Methodology
The hyperboloid, through neural stimuli, trains the individual in the triad, chewing, swallowing and breathing, in general for children and adults. The hyperboloid was created by orthopedic dentist Afrânio Pereira Cheida in 1989, as he noticed a lack of craniofacial growth and development in his patients. The hyperboloid has the consistency of hard, raw and dry foods [4].
The clinical case presented is from the private clinic of the professional responsible for this work in the city of Santa Barbara d' Oeste – SP.
Patient EFP 7 years old, with anterior open bite and muscular hypotonia, was prescribed hyperboloid exercises initially before the installation of the functional orthopedic appliance (AOF) Fig. 1.
The exercises are prescribed and taught during the consultation and repeated at home and return consultation once a week for correction of the exercises if necessary.
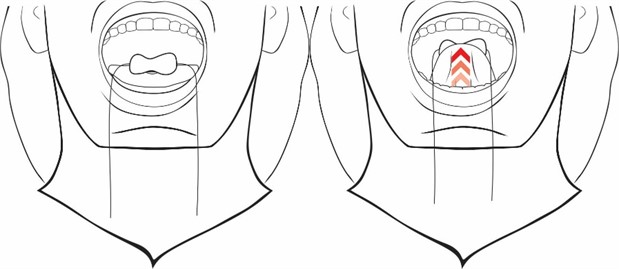
In Fig. 2, we observed an improvement in the interincisor distance, at the family’s request, the functional orthopedic device was not installed, we continued with the exercises and added the alternating unilateral chewing exercise for 3 minutes.
Fig. 108/2020, Initial intraoral frontal view of treatment with hyperboloid exercises

Fig. 210/2020 intraoral frontal view of the results achieved in 2 months of exercises

Fig. 303/2021, intraoral frontal view of the results achieved in 5 months of exercises

Patient stopped attending appointments for 2 years and 2 months, returning on 05/2023 Fig. 4. observing the results and carrying out functional examinations of laterality, protrusion, swallowing and chewing, the Simões Network 3 functional orthopedic device was installed to expand lateroprotrusive movements. During the functional examination, tongue interposition was observed during swallowing, protrusion showed a good interincisal relationship and chewing was inefficient.
Fig. 405/2023, intraoral frontal view after return after 2 years and 2 months

Fig. 507/2024 SN 3 just to sleep and continue with alternating unilateral chewing exercises. Alternating unilateral chewing exercises were prescribed based on the circuit theory of occlusal forces

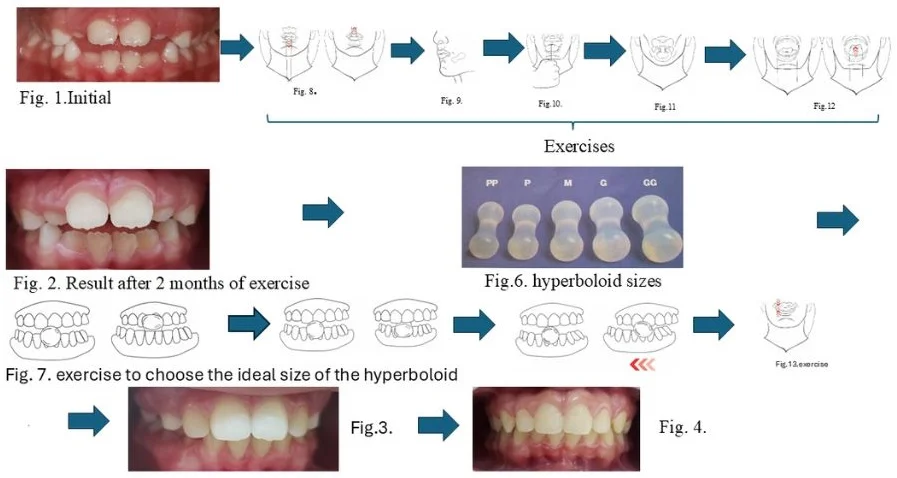
The hyperboloid is made of silicone and has 5 sizes, XS, S, M, L, XXL, Fig. 6 for muscle treatments we start from the smallest size to the largest. When chewing exercises are prescribed, you must choose the ideal size for each patient, placing the hyperboloid in the midline, holding it between the front teeth and making movements of protrusion, retrusion, right and left laterality, if there is tooth contact in these movements, choose the largest [10] Fig. 7.
Fig. 6Hyperboloid sizes.
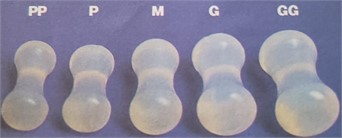
Fig. 7Movements required to choose the ideal size of the hyperboloid for chewing.

a) Protrusion
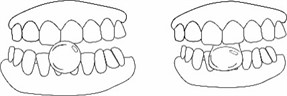
b) Retrusion
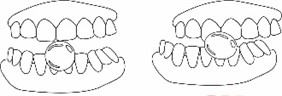
c) Laterality
Prescribed exercises are shown in Figs. 8-13.
Fig. 8Toning the upper and lower central orbicularis oris for 3 minutes, 3x a day, place the hyperboloid on the vestibular of the upper teeth, seal the lips and pull downwards and repeat on the lower one, pulling upwards
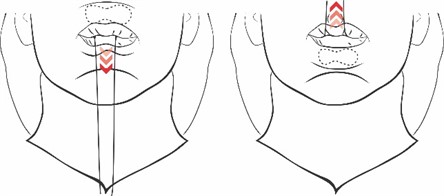
Fig. 9Toning the right and left buccinator for 3 minutes, 3 times a day, place the hyperboloid in the lower or upper buccinator region and use a suction movement to move the hyperboloid, 1 and a half minutes on each side

Fig. 10Toning the tongue with elastic, 10 movements 3x a day, tie a dental floss to the 3/8 orthodontic elastic at one end, place the tongue inside the elastic and the most posterior one and pull it forward until it comes out 10 times
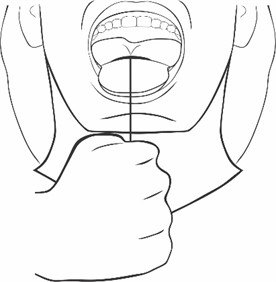
Fig. 11Orthodontic pacifier – rhythmic sucking movement 3 minutes 3x a day, makes a rhythmic sucking movement, this exercise was developed by speech therapist Beatriz Padovan, excites the functions for their own sake, the use of the pacifier in the exercise directed by parents and professionals does not deform the dental arches
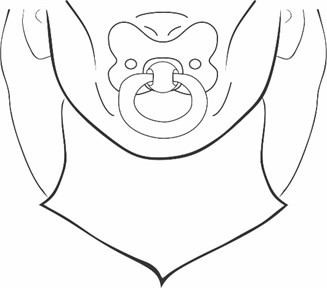
Fig. 12Stimulation of the tongue with a hyperboloid, place the hyperboloid on the tongue and pull it, closing the mouth, touching the palate and applying force with the tip of the tongue
3. Results
Patient had an improvement in muscular hypotonia with the prescribed exercises with hyperboloid Fig. 1, 2, 3, 4 and 5, with this an improvement in aesthetics, with the distance between incisors reduced, improvement in the quality of life reported by the family, eating better, sleeping better, at school he showed improvements in concentration.
Fig. 13Alternate unilateral chewing, 3 minutes 3x a day, chew the hyperboloid from one side to the other
4. Conclusions
The case report highlights the importance of adjuvant therapy with hyperboloid in functional jaw orthopedics, contributing significantly to stimulating the structures of the stomatognathic system, particularly in this case.
References
-
M. Rigon, “Ajuste oclusal no tratamento da mordida aberta anterior, Relato de caso clínico,” (in Portuguese), Monografia do curso de especialização do curso de ortopedia funcional dos maxilares, ACDC, Campinas, 2017.
-
L. Alves, Oclusão Ortopédica. (in Portuguese), São Paulo, Brasil: Editora Oclusivo, 2001.
-
V. Degan and R. M. Puppin-Rontani, “Remoção de hábitos e terapia miofuncional: restabelecimento da deglutição e repouso da língua,” (in Portuguese), Revista Pro – fono scientific update, Vol. 17, No. 3, p. 375, 2005.
-
A. Cheida, Instrumento De Mastigação Hiperboloide. (in Portuguese), São Paulo, Brasil: Editora Icone, 2004.
-
B. Padovan, “Deglutição atípica – reeducação mioterápica em pressões atípicas da língua: diagnóstico e terapia,” (in Portuguese), Revista Ortodontia, Vol. 9, No. 1, pp. 59–74, 1976.
-
W. Simões, P. Valerio, and D. Duarte, Ortopedia Funcional Dos Maxilares. (in Portuguese), Brasil: Quintessence Publishing, 2020.
-
P. Planas, Reabilitação Neuroclusal. (in Portuguese), Rio de Janeiro, Brasil, 1997.
-
R. S. Carvalho, J. E. Scott, A. Bumann, and E. H. K. Yen, Ciência E Prática Da Oclusão. São Paulo: Editora Quintessence, 2000.
-
C. R. Douglas, Fisiologia Aplicada À Fonoaudiologia. (in Portuguese), Rio de Janeiro, Brasil: Editora Guanabara Koogan, 2006.
-
F. Augusto Novo Borghi, R. Queiroz, and J. R. Gurgel Testa, “Treatment of traumatic facial paralysis with mechanical stimulus – hyperboloid: case report,” (in English), Jaw Functional Orthopedics and Craniofacial Growth, Vol. 1, No. 2, pp. 31–35, Dec. 2021, https://doi.org/10.21595/jfocg.2021.22027.
About this article

The authors have not disclosed any funding.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
The authors declare that they have no conflict of interest.
The representative gave written informed consent prior to the study.
