Abstract
Background: The aim of the study was to evaluate and compare destruction effect to different heart structures using RF, cryo and laser methodology in animal (pig) model. Methods: Ablation procedure was performed on right and left pulmonary veins area, free wall of right and left atrias, and free wall of ventricles positioning ablation electrode from endocardial side. Ablation electrodes were inserted through an incision in right/left auricle. The effects of ablation were observed visually and using thermography for temperature control. Results: Standard recommended parameters for both of used destruction energies were possible to evoke quick critical scar formation and rupture. Temperature in cardiac surface differs from 34.5 till 70.2 °C, and directly depends from electrode compression level, time of application and energy power. We express dissent from the general view, what destruction in cardiac structures is point like. We observed enough high range of temperature dispersion, especially in ventricles. Conclusions: Usage of thermography enable to estimate peculiarities and borders of destruction site, optimize parameters of ablation, allows us to avoid or minimize undesirable effects, save structures and improve clinical outcomes.
1. Introduction
Recently most of the cardiac rhythm disorders are corrected by transvenous way, using radiofrequency, microwave, laser energies or cryoablation. In over then 20 years of clinical experience, catheter radiofrequency ablation (RFA) has become standard and mostly developed approach. Unfortunately, despite of increased experience and using modern RFA technologies short- and long-range postoperative complications and relapses are nor rare, what make poor clinical outcomes [1-3]. Usage of cryoenergy is high effective, especially in atrial fibrillation correction procedures in pulmonary veins zone, but technically complicated and relatively expensive. Microwave weren’t useful in clinical practice because of huge thrombogenesis, uneven endocardial lesions and high perforation rate [4]. In the 1980s, were developed and tested successfully laser ablation methodology [5, 6]. The results showed that by using an open-irrigated laser catheter system, deep lesions can be achieved within seconds without thrombus formation or steam pop [7]. Recently, all this novel techniques develop optimization, are testing new catheter systems but subclinical are mostly used an isolated thigh-muscle model, which is far away from real clinical conditions. Aim of our study was in experimental model to test RF, cryo and laser ablation techniques, analyze possible mechanisms of complications, measure and determine optimal ablation parameters on beating pig heart.
2. Methods
12 female pigs (weight ~20-25 kg) used in experimental study. Hearts were exposed via sternotomy and pericardtomy, destruction of various heart areas was performed from the endocardial surface by inserting the electrode through femoral vein or the incision on the right or left auricle. For RFA standard 4 and 8 mm “Biosense Webster” (Johnson and Johnson,USA) intracardial electrodes were used. Destruction was performed using Prucka Engineering® RF energy generator OSYPKA HAT 200S. Destruction parameters: energy – 10-50 W, time – 10-60 sec. Cryodestruction was performed using cryoaplicator “Cryocauter KCH 450”. Cryodestruction parameters: atria – application time 1-2 min., temperature on the end of applicator –80 °C. For laser ablation we used loop form 10F electrode-laser catheter, which was inserted previously through the a. femoralis, position in the heart controlled by finger, ablation parameters – 20-35 W, 60 s.
Temperature changes in epicardial surface registered with thermo camera ThermaCAM P640, emission έ-0.98, temperature sensitivity ≤ 0.05°C. After destruction, damaged zones were excised and evaluated histologically. Three excised hearts were given for anatomorphological analysis – intracardial nervous tracts topography and state identification.
3. Results
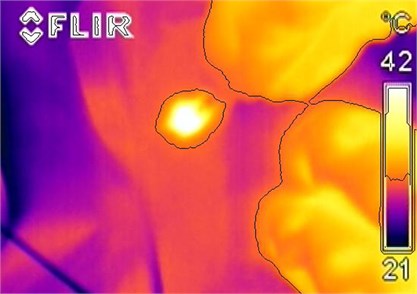
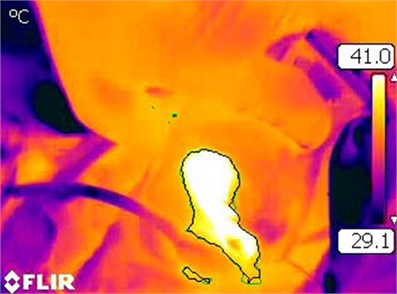
During RFA procedures on surface of atriums, destructive thermo effect (>46 °C) was observed after 5-7 s, after application, despite of power of energy and type of electrode. Dotted zone of total destruction using 20-30 W power and both type electrodes was 3-4 mm, whereas using 50 W – 4-6 mm. Partial destruction zone usually was equal or marginally, but regularly major than total destruction zone (Fig. 1(a)). Usually zone of destruction was ellipsoid, whereas temperature restoration occurred in 25-78 s., subject to power of energy, time of application and type of electrode. Peculiarities of RFA in site of pulmonary veins were similar comparing with free wall of atrium, however damage area was 20-30 percent greater and destruction site was like irregular ellipse pointed toward pulmonary veins flow to atrium. (Fig. 1(b)). 30 and 50 W 20-60 s applications outcomes were similar in total damage site, but partial damage sites differs significantly according to power and time of application.
Fig. 1a) Total and partial (marked) destruction zones in site of pulmonary veins ostium, using 20 s; 30 W power; b) the same using 20 s; 50 W power
a)
b)
Spread of RFE in ventricule wall had significant pecularities. We observed well marked temperature dispersion. Partial destruction zone went through myocardium and made 10-15 mm in width forming irregular oval with interstitial lines. This phenomenon was visible independent if RFA was made from endocardial or epicardial surface (Fig. 2).
Using cryoablation, destruction zone was total, even and forming regular oval. Destruction zone was statistically reliably even in all sites of heart and almost independent from application time (Fig. 3).
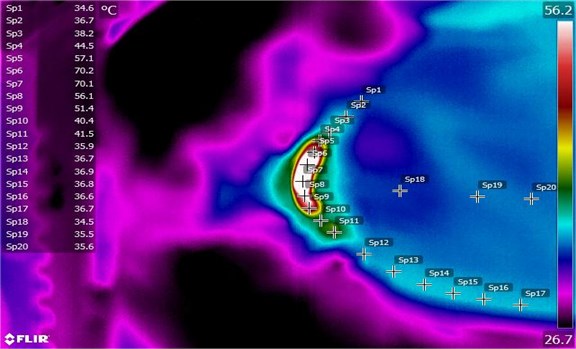
Using cryoablation approach, destruction zone was total, even and forming regular oval. Destruction zone was statistically reliably even in all sites of heart and almost independent from application time. The same we observed using laser ablation. The laser causes localized heating-up of the heart tissue, with temperature scale 34.1-70.2°C and enough restricted scar formation (Fig. 3).
Fig. 2Destruction in endocardial surface of left ventricule
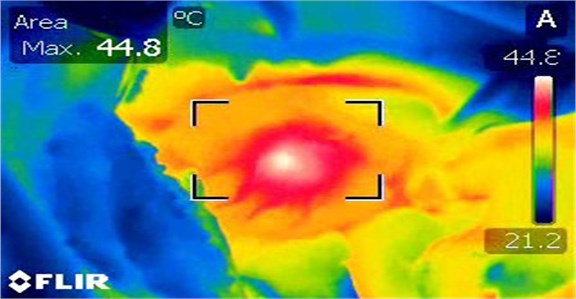
Fig. 3Thermogramm of laser destruction in site of pulmonary veins ostium, using 60 s and 35 W power
4. Conclusions
Usage of thermography enable to estimate peculiarities and borders of destruction site, optimize parameters of ablation, allows us to avoid or minimize undesirable effects, save structures and improve clinical outcomes.
References
-
Tan E. S., Mulder B. A., Rienstra M., et al. Pulmonary vein isolation of symptomatic refractory paroxysmal and persistent atrial fibrillation. Netherlands Heart Journal, Vol. 17, Issue 10, 2009, p. 366-372.
-
Ouyang F., Bansch D., Ernst S., Schaumann A., Hachiya H., Chen M., et al. Complete isolation of left atrium surrounding the pulmonary veins: new insights from the double-lasso technique in paroxysmal atrial fibrillation. Circulation, Vol. 110, 2004, p. 2090-2096.
-
Jais P., Hocini M., Hsu L. F., Sanders P., Scavee C., Weerasooriya R., et al. Technique and results of linear ablation at the mitral isthmus. Circulation, Vol. 110, 2004, p. 2996-3002.
-
Aupperle H., Doll N., Walther T., Ullmann C., Schoon H. A., Wilhelm Mohr F. Histological findings induced by different energy sources in experimental atrial ablation in sheep. Interactive Cardiovascular and Thoracic Surgery, Vol. 4, Issue 5, 2005, p. 450-455.
-
Weber H., Ischinger T. Cardiovascular application of Nd: YAG laser. Lasers in Surgery and Medicine, Vol. 4, 1988, p. 54-58.
-
Weber H., Enders S., Keiditsch E. Percutaneous Nd: YAG laser coagulation of ventricular myocardium in dogs using a special laser catheter. Pacing and Clinical Electrophysiology, Vol. 12, 1989, p. 899-910.
-
Ikeda A., Nakagawa H., Weber H., Sagerer-Gerhardt M., Sharma T., Pitha J. V., et al. Open-irrigated laser catheter produces deep lesions without thrombus or steam pop. PO1-83, Featured Poster Session and Reception, Heart Rhythm 32nd Annual Scientific Sessions, San Francisco, CA, USA, 2011.
About this article
