Abstract
This study evaluates maxillary changes in patients treated with jaw functional orthopedics through artificial intelligence and 3D technology, highlighting its advantages in precision and comfort. Growth changes in children aged 5-12 years after one year of treatment were analyzed using digital models and an intraoral scanner. The results showed significant changes in dental measurements and palatal rugaes, confirming the effectiveness of the treatment. Digital models proved to be superior to plaster models in durability and accuracy. Despite study limitations, such as the small sample size, the findings highlight the importance of 3D technology and suggest future directions for research in the area.
1. Introduction
In dentistry, artificial intelligence (AI) has been used to make the diagnostic process more accurate and efficient, in order to obtain better results. In jaw functional orthopedics (JFO), this system can help as an auxiliary tool to increase the accuracy of diagnosis, cephalometric analysis, and evaluation of the treatment plan [1].
The diagnosis and planning of jaw orthopedic functional treatment are traditionally done with plaster models, but, in recent years, 3D technology has evolved a lot and is incorporated into everyday practice, with the advantages that it does not break, has no alterations, and does not need physical storage. The use of intraoral scanners in dentistry for the reproducibility of teeth and dental arches has been a new trend in the last decade. In addition, it is a favorable option for children, as it brings significantly greater perception and comfort to the patient with intraoral scanners compared to the conventional method [2].
The 3D tooth surface model overlay is a powerful tool to evaluate changes occurred by growth, progress or the result of the treatment performed, having the palatal wrinkles and the palatine raphe as reference points in the model overlay study. Palatal rugaes are irregular ridges of connective tissue, located in the anterior portion of the palate, and are used as markers of personal identification. Rugaes are formed in the uterus in the third month and remain stable throughout life, with the exception of an increase in length due to normal growth [3].
The objective of this study was to evaluate the growth changes observed after 01 year of treatment with jaw functional orthopedics through dental and palatal rugae measurements analyzed using the 3Shape OrthoAnalyzer software.
2. Methodology
In this study, 59 children aged 5 to 12 years from the outpatient clinic of the JFO specialization course at the Jaw Functional Orthopedics Outpatient Clinic of the Brazilian Association of Dentistry, section Bahia (ABO-BA), located in the city of Salvador - Bahia, were initially used. The inclusion criteria were: patients treated at ABO-BA, children aged between 05 and 12 years, deciduous or mixed dentition with the presence of deciduous second molars, children with malocclusions. The exclusion criteria were: children who did not present a chronological age between 05-12 years, children with some special need that did not allow the use of the intraoral scanner, children without the deciduous second molar, children without malocclusions, children whose guardians did not sign the informed consent form. The children were scanned before and after 01 year of treatment with a functional orthopedic appliance (FOA) and, with the application of the exclusion criteria, 24 digital models of the upper arch were used.
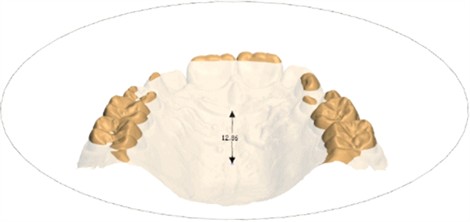
The 3Shape Trios 3 3D surface intraoral scanner from the Pierre Fauchard image radiology laboratory was used to obtain virtual models. The patients were scanned before and after functional orthopedic treatment and the digital models were analyzed using the 3Shape OrthoAnalyzer software, licensed for Compass 3D, where the following lines were marked: intercanine line - central region of the palatal cervical portion (Fig. 1); intermolar line of the second deciduous molars - midpalatine region (Fig. 2) papilla line to intercanine line (Fig. 3); palatine raphe line and occlusal plane (Fig. 4); and the length measurements of the first, second and third palatal rugaes (Fig. 5), about these lines, the initial measurements and measurements after 01 year of treatment were compared. All treatments were performed by the students from jaw functional orthopedic program at ABO-BA and only one examiner performed the children's intraoral scans and took the measurements using the OrthoAnalyzer software.
Fig. 1Intercanine line
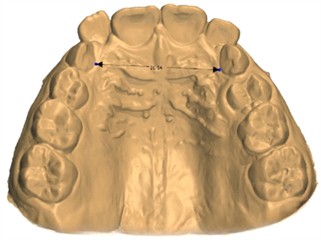
Fig. 2Intermolar line
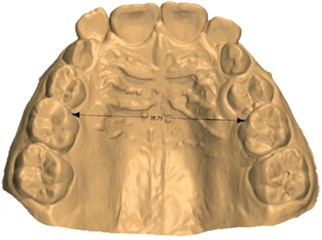
Fig. 3Papilla line to intercanine line
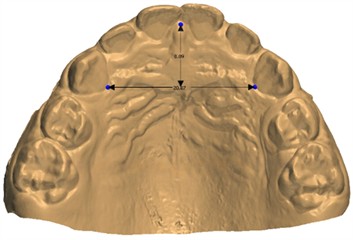
Fig. 4Palatine raphe line and occlusal plane
However, the sampling plan for this longitudinal experimental study, with a simple random sample composed of 1,200 patients aged 5 to 12 years and treated at the ABO-BA, has a maximum proportion of 0.5 with a 95 % confidence limit because the value of the proportion of the characteristic of the population under study is not known and it improves the precision of the estimates (Table 1).
Fig. 5First, second and third palatal rugaes
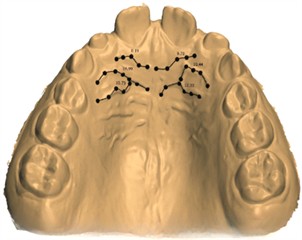
Table 1Sample calculation for different precisions (d)
d | 0.05 | 0.08 | 0.1 | 0.12 |
n. | 291 | 133 | 89 | 63 |
3. Results
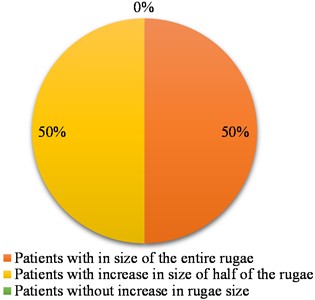
The results obtained were divided according to each of the lines measured in the digital models. Of the 12 patients included in the research, 67 % showed an increase in size in the measurements of the intermolar lines of the primary molars after 1 year of treatment (Fig. 6). In relation to the intercanine line, it was possible to observe an increase in size in 92 % of patients after 1 year of treatment (Fig. 7). For the lines: papilla line to intercanine line and palatal rafe line and occlusal plane an increase in size was observed in 33 % of patients after 1 year of treatment (Figs. 8 and 9). Finally, the results of the palatal rugae measurements found after the same treatment period were: for the first palatal rugae, 75 % of patients had an increase in the entire rugae, 17 % had an increase in just one of the two hemi-rugae and 8 % there was no increase in rugaes (Fig. 10); for the second palatal rugae, 75 % had an increase in size in the entire rugae and 25 % had an increase in just one of the two hemi-rugae (Fig. 11); for the third rugae, 50 % of patients had an increase in size in the entire rugae and 50 % had an increase in just one of the two hemi-rugaes (Fig. 12).
Fig. 6Intermolar line of decíduos second molars (mesio-palatal region)
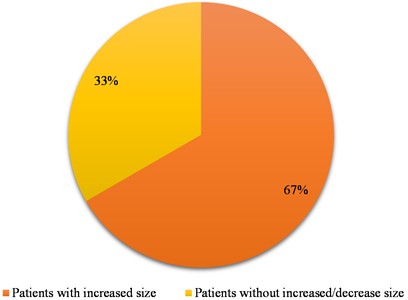
Fig. 7Intercanine line (central region of the cervical-palatal portion)
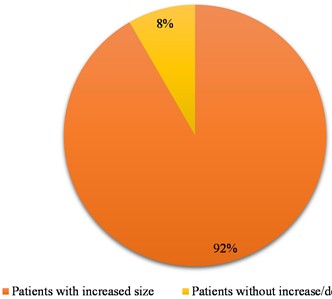
Fig. 8Papilla line to intercanine line
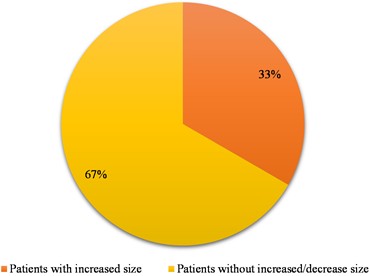
Fig. 9Palatal rafe line and occlusal plane
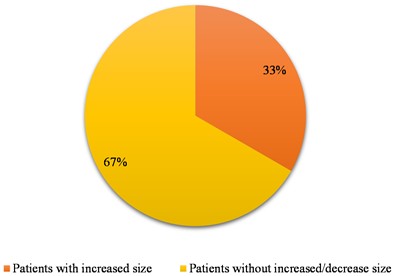
Fig. 10First palatal rugae
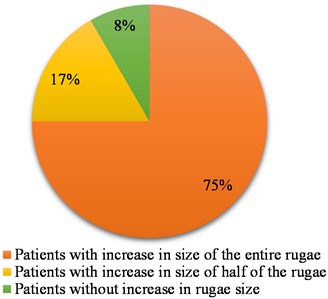
Fig. 11Second palatal rugae
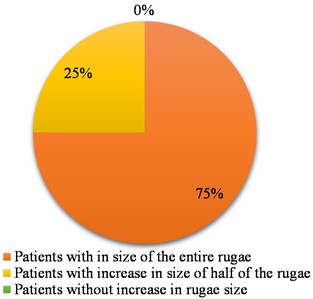
Fig. 12Third palatal rugae
4. Discussion
A recent study revealed significant changes in the dental and palatine rugae region measurements of the 3D digital models after one year of treatment with Jaw Functional Orthopedics, reinforcing the effectiveness of the treatment in modulating craniofacial growth. These results align with previous findings, highlighting the treatment's ability to induce measurable morphological changes in facial development, corroborating previous studies [4, 5].
Digital models offer several significant advantages compared to traditional models. They do not require physical storage space, have a lower acquisition cost, and are not subject to degradation due to aging, breakage, or loss. The use of intraoral scanning, which creates digital files of dental arches, a validated and considered adequate tool, is arousing the interest of dentists for the analysis, diagnosis, planning, and execution of clinical procedures. The introduction of digital models enables the evaluation of tooth movements through the superimposition of models from two or more moments, a process impossible with traditional plaster models. Thus, three-dimensional evaluation of tooth movements is already a consolidated reality [6].
Intraoral palate scan comparison holds potential for reliable human identification, even in a real-life scenarios, in a population of young adults whose palate may change. Additionally, the anterior area proves to be a good candidate for identification purposes, due to its inclusion in ante mortem scans and high reproducibility. Conversely, the digitization of physical impressions using plaster casts is considered an unreliable method for comparing palatal features [7].
Some authors evaluated the reliability of three-dimensional maxillary dental changes using two methods of digital-model superimposition. The maxillary digital dental models of patients with normal occlusion superimposed on palatal rugae, demonstrated adequate reliability for comparison at 5-year intervals using reference points or regions of interest. However, measurements taken with an interval of 40 years using both superimposition methods showed reproducibility below the acceptable level [8]. The 3D anatomical morphology of the palatine rugae area is not affected by specific dental treatments, indicating that it can maintain its morphological patterns of individuality even after undergoing rapid maxillary expansion. The absence of statistically significant differences between the pre- and post-treatment models supports the reliability of forensic applications based on the comparison of the morphology of palatal rugae [9].
In orthodontics, palatine rugae are often used as a reference for superimposing maxillary models and are considered the most stable landmarks of the oral cavity. However, they can be influenced by palatine expansions, which are common procedures to create space for crowded teeth. It is important to note that palatal expansions can significantly alter the morphology of palatal rugae. After a palatal expansion, human identification and sequential superimposition based on palatal rugae should be performed with care, especially immediately after the procedure, due to changes in the rugae’s position. Although palatal rugae generally maintain their stable shape and number, studies indicate that rapid maxillary expansion can alter their position, while slow maxillary expansion does not appear to have a discernible effect on the palatal rugae pattern in growing individuals [10].
Evidence suggests that functional orthopedic treatment of the jaws can influence craniofacial growth through different mechanisms, such as bone remodeling induced by orthopedic forces and improvement in muscle posture and function [11]. Understanding these processes is essential for refining therapeutic approaches and optimizing patient outcomes. Furthermore, other authors have examined changes in the width of the dental arch changes throughout development, addressing how factors such as age and continuous growth influence dentofacial morphology. One study concluded that between 6 weeks of life and 2 years of age, before the complete eruption of the deciduous dentition, significant increases occur in the widths of the anterior and posterior maxillary and mandibular arches in boys and girls. Between 3 and 13 years of age, both maxillary and mandibular arches exhibit significant increases in the intercanine and intermolar widths. However, after the complete eruption of the permanent dentition, a slight decrease is observed in the widths of the dental arches, more pronounced in the intercanine than in the intermolar width. The lower intercanine width stabilizes after the eruption of the canines. This study emphasizes the complexity of maxillary development throughout life and the need to consider these factors in the evaluation of orthopedic treatment results [12].
5. Conclusions
This pilot study demonstrated that the application of 3D technology and intraoral scanning in patients treated with Jaw Functional Orthopedics offer significant advantages in terms of accuracy, durability and comfort for patients, especially children. Analyses of growth changes after one year of treatment revealed significant changes in dental measurements and palatal rugae, confirming the efficacy of functional orthopedic treatment of the jaws in modulating craniofacial growth. The advancement of 3D technology and the use of AI will continue to play crucial roles in optimizing treatments, improving patient outcomes, and contributing to the development of modern dentistry.
References
-
S. B. Khanagar et al., “Developments, application, and performance of artificial intelligence in dentistry – A systematic review,” Journal of Dental Sciences, Vol. 16, No. 1, pp. 508–522, Jan. 2021, https://doi.org/10.1016/j.jds.2020.06.019
-
D. Serrano-Velasco, A. Martín-Vacas, M. M. Paz-Cortés, G. Giovannini, P. Cintora-López, and J. M. Aragoneses, “Intraoral scanners in children: evaluation of the patient perception, reliability and reproducibility, and chairside time-A systematic review,” Frontiers in Pediatrics, Vol. 11, p. 1213072, Jun. 2023, https://doi.org/10.3389/fped.2023.1213072
-
E. Henninger, G. Vasilakos, D. Halazonetis, and N. Gkantidis, “The effect of regular dental cast artifacts on the 3D superimposition of serial digital maxillary dental models,” Scientific Reports, Vol. 9, No. 1, Jul. 2019, https://doi.org/10.1038/s41598-019-46887-1
-
A. M. Araújo and P. H. Buschang, “The effects of functional appliances on the transverse dimension of the maxila and mandible,” (in Portuguese), Revista Dental Press de Ortodontia e Ortopedia Facial, Vol. 10, No. 2, pp. 119–128, Apr. 2005, https://doi.org/10.1590/s1415-54192005000200015
-
R. Bernardes, L. M. Di Bisceglie Ferreira, A. J. Machado Júnior, and M. H. Jones, “Effectiveness of functional orthopedic appliances as an alternative treatment among children and adolescents with obstructive sleep apnea: Systematic review and meta-analysis,” Sleep Medicine, Vol. 105, pp. 88–102, May 2023, https://doi.org/10.1016/j.sleep.2023.03.008
-
M. A. Anacleto and B. Q. Souki, “Superimposition of 3D maxillary digital models using open-source software,” Dental Press Journal of Orthodontics, Vol. 24, No. 2, pp. 81–91, Apr. 2019, https://doi.org/10.1590/2177-6709.24.2.081-091.bbo
-
A. Mikolicz, B. Simon, O. Gáspár, A. Shahbazi, and J. Vag, “Reproducibility of the digital palate in forensic investigations: a two-year retrospective cohort study on twins,” Journal of Dentistry, Vol. 135, p. 104562, Aug. 2023, https://doi.org/10.1016/j.jdent.2023.104562
-
D. Garib et al., “Superimposition of maxillary digital models using the palatal rugae: Does ageing affect the reliability?,” Orthodontics and Craniofacial Research, Vol. 22, No. 3, pp. 183–193, Apr. 2019, https://doi.org/10.1111/ocr.12309
-
V. Lanteri et al., “Assessment of the Stability of the Palatal Rugae in a 3D-3D Superimposition Technique Following Slow Maxillary Expansion (SME),” Scientific Reports, Vol. 10, No. 1, Feb. 2020, https://doi.org/10.1038/s41598-020-59637-5
-
S. Santhosh Kumar, R. Chacko, A. Kaur, G. Ibrahim, and D. Ye, “A systematic review of the use of intraoral scanning for human identification based on palatal morphology,” Diagnostics, Vol. 14, No. 5, p. 531, Mar. 2024, https://doi.org/10.3390/diagnostics14050531
-
M. E. A. Nascimento, S. R. A. Veras, G. R. P. Santos, G. S. G. D. Silva, and S. M. S. D. Silva, “Functional orthopedic jaw therapy in the treatment of angle class III in a child patient,” (in Portuguese), Odontologia Clínico-Científica, pp. 175–179, 2020.
-
S. E. Bishara, D. Ortho, J. R. Jakobsen, J. Treder, and A. Nowak, “Arch width changes from 6 weeks to 45 years of age,” American Journal of Orthodontics and Dentofacial Orthopedics, Vol. 111, No. 4, pp. 401–409, Apr. 1997, https://doi.org/10.1016/s0889-5406(97)80022-4
About this article

The authors have not disclosed any funding.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Camila Cruz Rocha: Participation in conceptualization, project administration, investigation, resources, writing original draft, review, and editing. Luanda Gomes: visualization. Bruno Gribel: software programing. Marcos Gribel: supervision. Maria Rita Sancho: Project administration, supervision.
The authors declare that they have no conflict of interest.
As it is a pilot project, this project will still be reported on the Brazil Platform.
