Abstract
This study aimed to evaluate the number, intensity and position of occlusal contact points in a case of mesiocclusion, hyperdivergence, with open bite. An occlusal record was taken from a patient with anterior and lateral open bite mesiocclusion, using the Planmeca Esmerald S intraoral scanner in maximum intercuspation. The intensity of the occlusal contact was analyzed with the software 3shape Ortho Analyzer Orthodontics, using the Occlusion Map module, through the 3D Color Map tool, with a 0.5 mm virtual articular paper. These results were compared to the occlusal support points defined by Planas [10]. The interpretation of the data obtained was made by assessing the interocclusal intensity of the contact points, number of contacts and position during three different moments (1S, 2S, 3S) in the record taking process. The chromatic scale of the Color Map is: red, orange, yellow, green and blue. To identify the occlusal contact points in digital, they are shown in red points when full contact occurs, while minimum contact is shown in blue. We evaluated the number of teeth with interocclusal contacts. It was determined that having the appropriate number of contacts does not imply that they are in the correct position. In addition, the method suggests reliability in the filing and record keeping of occlusal contacts. By identifying intensity, number and position of the occlusal support point we can objectively record interocclusal alterations.
Highlights
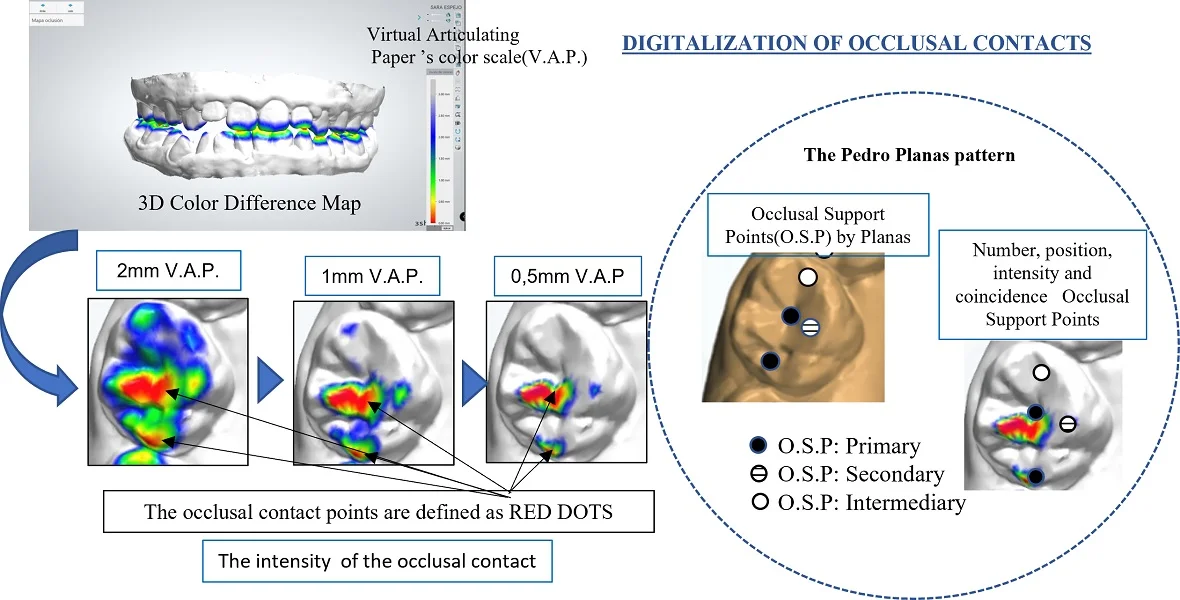
- The occlusal contact points are defined as RED DOTS.
- The intensity of the occlusal contact belongs to Virtual Articulating Paper ’s color scale.
- The occlusal support points established by Planas according to his Neurocclusal Rehabilitation (NOR), are called: primary, secondary, and intermediate.
- the occlusal contact can be taken as opposite contacts in the elevation of the mandible.
- The digital models for the quantification of occlusal contacts represent a reliable and valid method to determine the exact position of occlusal contacts.
- The record obtained by dental scanner was saving in STL (Standard Triangle Language) file.
1. Introduction
It is possible to know the status of the occlusal contact using digital images through the intraoral scanner. This allows us to obtain a reliable occlusion record, which is an important point to consider when we are going to interpret and/or transfer this information to the laboratory, so it can be objective and reproducible. The clinical records and data transfer in which waxes and other bite recording materials are used, have disadvantages related to inaccuracy and handling problems [1].
The current use of the dental scanner in dental practice contributes to conventional methods [2], in the interpretation of the quality of occlusal records, such as those obtained through articulating paper [3]. Because it is a noninvasive method with no radiation exposure, digital scanning is expected to reduce treatment time and improve treatment quality by allowing frequent evaluations as needed [4]. In that sense, this technology allows the virtual occlusal registration methodology to become increasingly common in dental practice [5].
Traditionally, articulating paper with different thicknesses has been adopted as the Gold Standard for analyzing occlusal contacts, directly on patients or on plaster models [6]. Occlusal contacts are defined as the contact of opposing teeth in elevation of the mandible, which increase in number as the dental arches come together in occlusion until reaching the maximum intercuspal position (MIP). This position contributes to maintaining a precise alignment of the arches, to masticatory efficiency and facilitates the diagnosis and planning of restorative procedures.
Occlusal contacts provide information for diagnosis and treatment prognosis. Knowing the location, number and extension area of these contacts is ideal to assess the presence of occlusal interferences and/or premature contacts that can lead to changes in the supporting tissues of the teeth, masticatory muscles, mandibular posture and TMJ [7]. The distribution and area of occlusal contacts can be analyzed through three digital analysis methods (Fig. 1) incorporated into the 3Shape Occlusion Map software. These methods are: “3D Color Difference Map” (Fig. 1(a)), Spot Analysis (Fig. 1(b)) and Virtual Analysis (Fig. 1(c)), which can provide reliable and accurate analysis results of the occlusal contact distribution and the occlusal contact area of the dental model [8].
The 3D color map in 3shape Ortho Analyzer Orthodontics 2020 Software has a chromatic scale: red, orange, yellow, green, and blue. Red represents the strongest contact and blue, that of the least contact [9].
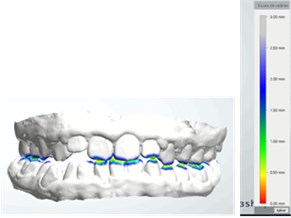
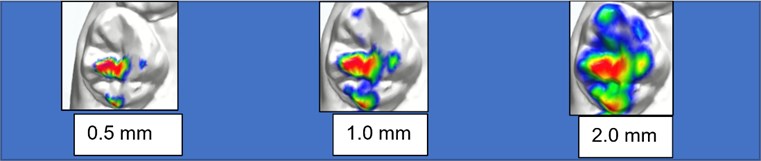
The occlusion map allows to evaluate the intensity [6] of the occlusal contact, through the virtual articulating paper thickness tool: It ranges from 0 mm to 4 mm (Fig. 2).
Fig. 1Three digital analysis methods
a) 3Shape occlusion map software
b) Spot analysis
c) Virtual articulating paper’s color scale
Fig. 2Occlusal contact at different thicknesses on the tooth: same tooth, same case
2. Objective of the study
To evaluate the number, intensity and position of the occlusal contact points in a case of mesioclussion with hyperdivergence and anterior and bilateral open bite (Fig. 4).
2.1. Materials and methods
A case of a patient who required the continuation of their care in Functional Maxillary Orthopedics was selected.
The intraoral scanner used for this study was the Planmeca® Esmerald S. The interocclusal record of the maxilla and mandible is taken and then, in maximum intercuspation, the left and right bite. The interocclusal adjustment happens automatically.
The reference record was analyzed with the 3Shape Ortho Analyzer Orthodontics 2020 software, and the “Occlusion Map” was used as a tool to evaluate occlusal contacts. This map assesses the intensity of the occlusal contact through the color scale that corresponds to the thickness of the virtual articulating paper, which ranges from 0 to 4 mm. In the present study, the analysis was done using a virtual articulating paper of 0.5 mm. The occlusal contact points are defined as red dots on the digital models, and these were the ones evaluated.
These dental contacts in red were compared with the occlusal support points established by Planas [10] according to his Neurocclusal Rehabilitation (NOR), which he called: primary, secondary, and intermediate.
Supports that maintain the vertical dimension in the position of maximum intercuspation:
– Primary: upper and lower incisors, canines and molars.
– Intermediates: Mesio-vestibular cusp of the lower 1st molar occluding against the interproximal ridge of the 2nd premolar and upper 1st molar.
– Secondary: They also maintain the vertical dimension, but with less power [10].
Fig. 3Occlusal support contacts (O.S.C.)

2.2. Data collection
In a clinical case, the disjunction splint treatment associated with Petit’s Mask and orthopedic elastics was withdrawn after 9 months, according to Raymond Jean Louis Therapeutics for hyperdivergence [11], to a female patient aged 14 years and 7 months with a previous diagnosis of hyperdivergence, mesioclusion, anterior and bilateral open bite. The intraoral scan is performed in order to evaluate the contact points that she may have in the posterior and anterior sector.
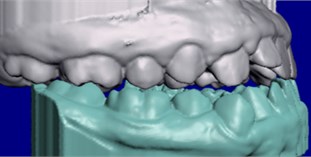
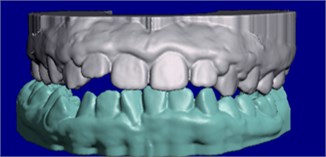
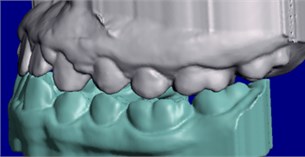
The Planmeca Esmerald S intraoral scanner was used. The intraoral camera was placed in the mouth with the help of a retractor. Images of the mandibular and maxillary teeth were taken, and maximum intercuspation bite registrations (MIP) were obtained with saliva-dried teeth, right and left, respectively. The record obtained was reevaluated before saving the file, the maximum virtual and real intercuspation were compared, and a model file was generated in STL (Standard Triangle Language) (Fig. 4).
Fig. 4STL models generated by the first intraoral scan
The patient's dental files and occlusal records were collected at 3 different moments (Fig. 5): 1st scan (1S) after removal of the disjunction splint (Fig. 5(a)), 2nd scan (2S) 3 months after using the Simoes Network 3 (SN3) Functional Orthopedic Appliance (FOA) (Fig. 5(b)) and 3rd scan (3S) after 2 months with the use of an upper occlusal splint for chewing (Fig. 5(c)) combined with the SN3 in a total period of 7 months.
The evaluation of the data obtained was visual, observing the occlusal interaction, the number of contact points in red through a color map in the 3D models, and the position of the contact points in relation to the occlusal supports established by Planas. Fig. 5(c) Chewing splint.
Fig. 5The patient's dental files and occlusal records

a) Disjunction splint

b) F.O.A SN3

c) Chewing splint
3. Results
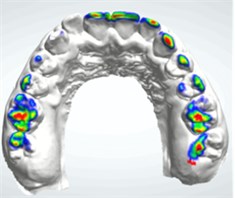
In Fig. 6 we observe the contact points obtained in the upper jaw, in the three scans using the Occlusion Map.
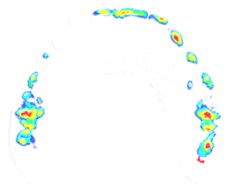
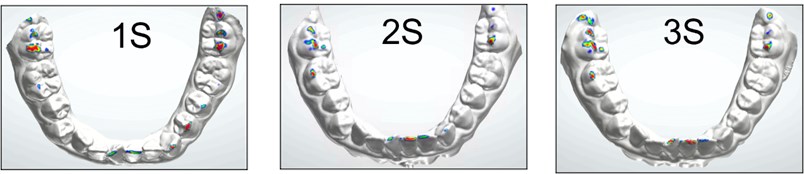
In Fig. 7 we observe the contact points obtained in the lower jaw in the three scans using the Occlusion Map.
Fig. 6The contact points obtained in the upper jaw in the three scans
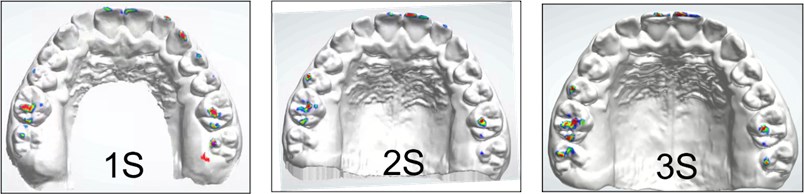
Fig. 7The contact points obtained in the lower jaw in the three scans
Although the occlusal contact can be taken as opposite contacts in the elevation of the mandible, in open bites it is presented in an unusual way, because in these cases, the lack of occlusal contact is found in certain or specific supporting teeth.
In Fig. 8 we evaluated the number of teeth with interocclusal contacts and obtained in the upper jaw: 1S: 6, 2S: 5, and 3S: 8 teeth with red contacts (Fig. 8(a)) out of 14 teeth, and in the lower jaw 1S: 6, 2S: 5 and 3S: 7 teeth with red contacts (Fig. 8(b)).
Fig. 8The number of teeth with interocclusal contacts
a) Upper jaw red contacts
b) Lower jaw red contacts
Fig. 9 shows the percentage of all teeth with red contact in the three scans: 1S:43 %, 2S:36 %, 3S:57 % for the upper jaw and 1S:43 %, 2S:36 for the lower jaw, respectively having 14 teeth in each arch. This shows us how the dental support was increasing from the beginning until the third scan.
Fig. 9The percentage of all teeth with red contact in the three scans.
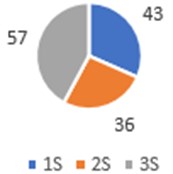
a) Upper jaw
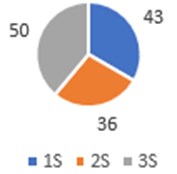
b) Lower jaw
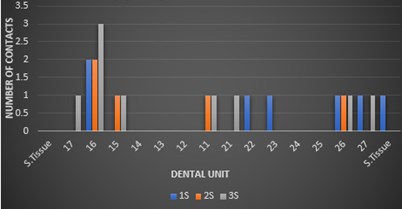
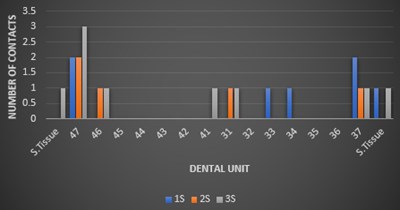
When taking records at separate times of treatment, the number of occlusal contacts varied; it was higher in the molar region, followed by the anterior region and very little or almost nothing in the premolar area, which is characteristic of the type of skeletal problem of the patient. In the 1S, only 47 % of the upper maxilla and 43% of the mandible present red contacts in the posterior area, and in the 2S, even when these contacts are reduced to 36 % in the upper maxilla and 36 % in the mandible, shows reds contact in the incisor area, important in this clinical case. According to Planas, incisor contact must be present at certain development stages of the stomatognathic system and in the physiological movement of mandibular dynamics, however for this author the absence or undue of incisor contact can cause periodontal problems [10]. In the 3S with 57 % in the upper maxilla and 50 % in the mandible, an increase in the number of red contacts is manifested, giving an indicator that the functional orthopedic treatment has a good performance.
Fig. 10The number of occlusal contacts
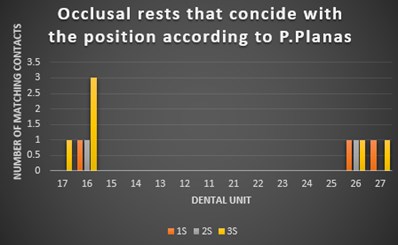
a) Coincident occlusal rests upper jaw
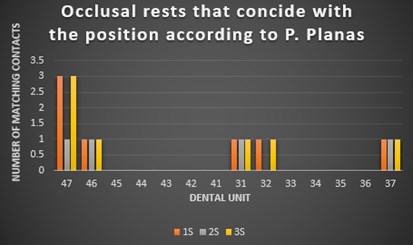
b) Coincident occlusal rests lower jaw
Fig. 10 shows that the number of occlusal contacts that should coincide, according to the Pedro Planas pattern, is higher in the lower jaw (Fig. 10(b)) than it is in the upper jaw (Fig. 10(a)). However, there was a significant difference in the lower anterior region compared to the upper one. The red contacts on the upper one are not in the right position according to Planas, but for this case of hyperdivergence it is good, although it is not adequate.
Similarly, the C.O.R. are absent in the premolar area. The greatest number of suitable contacts were located in the area of the upper and lower molars.
We were also able to observe that, even though the red contacts decreased in the second scan, they appeared in the correct position in the third scan, which indicates that our treatment is on the right track.
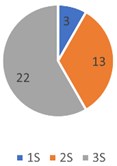
In Fig. 11 we express these results in percentages, and we have that 1S:9 %, 2S:6 %, 3S:19 % represent the upper jaw, and 1S:3 %, 2S:13 %, 3S:22 % in the lower jaw, out of the 36 occlusal support points that, according to Planas, must exist in each maxilla. The coincidence of red contacts and occlusal support is very low. Digital analysis can provide reliable and accurate analysis results of the occlusal contact distribution and occlusal contact area in the digital model, the results obtained by this method can serve as a reference for the design of the required functional orthopedics appliance due to the clinical occlusal analysis [8].
Currently, there is still no Gold Standard regarding digital occlusal analysis, articulating paper is still preferred due to its low cost and ease of use [12].
Fig. 11Percentages of the coincidence whit red contacts
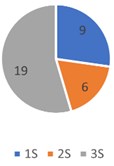
a) Upper jaw
b) Lower jaw
4. Discussion
This study demonstrated that digital models for the quantification of occlusal contacts represent a reliable and valid method to determine the exact position of occlusal contacts.
We have found that the interocclusal contact in the position of maximum intercuspation is also found in the retromolar area, which is demarcated with this system of virtual occlusal contacts, given that the use of conventional articulating paper does not allow visualization or later analysis of these contacts.
Although there have been many reports on the reliability and validity of different digital programs, few have considered occlusal contacts as a variable, and no study has used clinical records as control [13].
These inadequate contacts can produce negative effects on the periodontium, teeth, muscles, and TMJ. In our case, these objective records of the occlusal contacts allow us to create the appropriate design of the required functional orthopedic appliance. Chewing patterns induce adaptation of the periodontal tissue through occlusal contact.
Chewing movements that deviate from normal chewing movements will increase the mobility of the group of teeth involved. The relation between periodontal attachment/bone loss and occlusal trauma may provide important insights into the central dilemma of occlusal trauma and periodontal disease [14].
5. Conclusions
Although there are currently no parameters for digital occlusal analysis regarding the size of the contact area, the intensity of the color in the thickness of the virtual articulating paper and the position of the contact point, more studies are required in this regard to establish the Gold Standard of this methodology.
Despite the limitations of the present clinical case, the results suggest greater reliability to record occlusal contacts with digital methods using the intraoral scanner and saving the information in STL files.
Different occlusal relationships can affect the number, magnitude, and position of tooth contacts.
Training and understanding are required for the use of these new digital tools, since soft tissue contact is not reported in the literature as part of the occlusal plane and can influence mandibular position.
Therefore, this analysis is important to study occlusal relationships before, during and after treatment. In the area of functional maxillary orthopedics, this analysis would contribute to determining contacts that allow us to identify postural alterations of the mandible in its relationship with the maxilla and the functioning of the teeth in the arches according to their contacts in red; this would allow us to identify the different movements that are required in the stomatognathic system to optimize our treatments.
References
-
A. Sharma, G. Rahul, S. Poduval, K. Shetty, B. Gupta, and V. Rajora, “History of materials used for recording static and dynamic occlusal contact marks: a literature review,” Journal of Clinical and Experimental Dentistry, Vol. 5, No. 1, pp. e48–53, 2013, https://doi.org/10.4317/jced.50680
-
F. G. Mangano, G. Veronesi, U. Hauschild, E. Mijiritsky, and C. Mangano, “Trueness and precision of four intraoral scanners in oral implantology: a comparative in vitro study,” PLOS ONE, Vol. 11, No. 9, p. e0163107, Sep. 2016, https://doi.org/10.1371/journal.pone.0163107
-
E. Solaberrieta, J. R. Otegi, N. Goicoechea, A. Brizuela, and G. Pradies, “Comparison of a conventional and virtual occlusal record,” The Journal of Prosthetic Dentistry, Vol. 114, No. 1, pp. 92–97, Jul. 2015, https://doi.org/10.1016/j.prosdent.2015.01.009
-
H. Lee, J. Cha, Y.-S. Chun, and M. Kim, “Comparison of the occlusal contact area of virtual models and actual models: a comparative in vitro study on Class I and Class II malocclusion models,” BMC Oral Health, Vol. 18, No. 1, pp. 1–9, Dec. 2018, https://doi.org/10.1186/s12903-018-0566-7
-
E. Solaberrieta, A. Arias, A. Brizuela, X. Garikano, and G. Pradies, “Determining the requirements, section quantity, and dimension of the virtual occlusal record,” The Journal of Prosthetic Dentistry, Vol. 115, No. 1, pp. 52–56, Jan. 2016, https://doi.org/10.1016/j.prosdent.2015.06.013
-
C. Fraile, A. Ferreiroa, M. Romeo, R. Alonso, and G. Pradíes, “Clinical study comparing the accuracy of interocclusal records, digitally obtained by three different devices,” Clinical Oral Investigations, Vol. 26, No. 2, pp. 1957–1962, Feb. 2022, https://doi.org/10.1007/s00784-021-04174-2
-
M.-Y. Jeong, Y.-J. Lim, M.-J. Kim, and H.-B. Kwon, “Comparison of two computerized occlusal analysis systems for indicating occlusal contacts,” The Journal of Advanced Prosthodontics, Vol. 12, No. 2, pp. 49–54, 2020, https://doi.org/10.4047/jap.2020.12.2.49
-
N. Xiao, Y. C. Sun, Y. J. Zhao, and Y. Wang, “Preliminary study on three digital analysis methods for analyzing the distribution and area of occlusal contacts,” Journal of Peking University, Vol. 52, No. 1, pp. 144–151, 2020.
-
K. P. Botsford, M. C. Frazier, A. A. M. Ghoneima, A. Utreja, S. S. Bhamidipalli, and K. T. Stewart, “Precision of the virtual occlusal record,” The Angle Orthodontist, Vol. 89, No. 5, pp. 751–757, Sep. 2019, https://doi.org/10.2319/092018-684.1
-
P. Planas, Rehabilitación Neuro-Oclusal (RNO). Barcelona: Ediciones Científicas y Técnicas, 1994.
-
R. J. Louis, “Tratamiento Ortopédico de las maloclusiones de Clase III. Rehabilitación oclusal y funcional. Tain l hermitage: Coté Impression,” 2004.
-
S. E. Bostancıoğlu, A. Toğay, and E. Tamam, “Comparison of two different digital occlusal analysis methods,” Clinical Oral Investigations, Vol. 26, No. 2, pp. 2095–2109, Feb. 2022, https://doi.org/10.1007/s00784-021-04191-1
-
J. Sigvardsson, S. Nilsson, M. Ransjö, and A. Westerlund, “Digital quantification of occlusal contacts: a methodological study,” International Journal of Environmental Research and Public Health, Vol. 18, No. 10, p. 5297, May 2021, https://doi.org/10.3390/ijerph18105297
-
S. Ishigaki, T. Kurozumi, E. Morishige, and H. Yatani, “Occlusal interference during mastication can cause pathological tooth mobility,” Journal of Periodontal Research, Vol. 41, No. 3, pp. 189–192, Jun. 2006, https://doi.org/10.1111/j.1600-0765.2005.00856.x
About this article

The authors have not disclosed any funding.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
The authors declare that they have no conflict of interest.
The research met all applicable standards for the ethics of experimentation. Participants provided written informed consent prior to the study.
