Abstract
The decrease in magnitude of maxillary dental anomalies at the primordial prevention level by using direct tracks, in addition to occlusal adjustments and masticatory guidance, has several features that can prove to be advantageous. The objective is to demonstrate how continuous in-person and online training performed by specialists in orthodontics and functional maxillary orthopedics of the Regional Hospital of Talca in the Maule region of Chile for odontologists in primary health care can be used to treat occlusopathy in its early stages. The cranial-cervical-mandibular system relies on genetic, environmental and functional factors for its development and the absence of functional stimuli can cause growth disturbances and malocclusions. The major advantage of Planas direct tracks is that it does not require patient collaboration because its basis is in selective wear and restoration with composite resin that acts continuously after construction. Additionally, it is low cost because sophisticated materials are not necessary for its execution and it is a simple technique that can be performed by general dentists, so it is not necessary to be a specialist in orthodontics.
1. Introduction
Malocclusion is an abnormal craniofacial relation [1, 8] and/or disorder that can affect aesthetics, function, facial harmony and psychological well-being. Its presence can directly impact the quality of life of a person [1]. Functional maxillary orthopedics uses neuro-occlusal rehabilitation (NOR) to study how and when to act on the neural receptors that provide the developmental response of the stomatognathic system, ensuring that they receive the physiological stimuli that is necessary for a normal and balanced developmental response [2]. In accordance with neuro-occlusal rehabilitation (NOR) [3], facial development is driven mainly by genotypic factors that give individuals unique features, such as those that are inherent to their race, family traits, etc. Telemedicine has made inroads in healthcare through the use of information (IT) and communications technology (Wi-Fi), providing online care to patients. After one year, teleorthodontics was implemented under teleodontology by the Office for Digital Health of the Ministry of Health of Chile as an asynchronous oral health strategy. This has been a valuable experience for the country in terms of public health, increasing access for the population with a focus on equity. The use of IT and Wi-Fi tools has strengthened the public healthcare network by enabling the application of therapeutic techniques commonly used in functional maxillary orthopedics and neuro-occlusal rehabilitation (NOR). Among these are Planas direct tracks, created by Spanish oral surgeon Dr. Pedro Planas, who inferred the growth laws of the stomatognathic system through the knowledge of physiological functions, mainly mastication, and the management of the vertical dimension of dental occlusion, which allows using it as a valuable resource in the early treatment of malocclusion [3, 6].
2. Methodology
This strategy allowed the odontologists of primary health care centers to train to prioritize and treat patients with primary dentition with maxillary dental anomalies, sometimes preventing referrals to more advanced care facilities – a benefit for patients from remote locations [6]. Odontologists attend in-person and online training sessions and upload extra and intra-oral panoramic X-rays and clinical photos to a digital platform where orthodontic specialists and functional orthopedists examine each case individually, creating PowerPoint presentations with images and charts [5]. This process includes training in direct track techniques for the treatment of anterior crossbites (inverted) with resin increments on crossed temporal teeth and unilateral or bilateral bites, and in Class II the inclinations of direct tracks are indicated by diagrams and schematics based on photographs of the patients. This knowledge allows odontologists of the CESFAMs (Family Health Care Centers) and CECOSFs (Community Health Care Centers) to learn from diagnostics and initial treatments, intercepting occlusopathy in primary dentition [6]. They also learn about correcting harmful habits such as unilateral mastication, oral breathing and atypical swallowing, which contribute to the formation of malocclusions [5, 7]. Planas direct tracks make the occlusal plane parallel with the Camper’s plane (from the inferior edge of the ala of the nose to the upper edge of the tragus) and regulate the vertical dimension [9]. The height of the Planas direct tracks is obtained by guiding the odontologists to create bite registrations with utility wax and silicone putty in the same manner that a removable appliance is made. These tracks are easily created, provide immediate results, and are prescribed for crossbites, overbites and distoclusion [4, 8]. The specialists of the Regional Hospital of Talca and the Regional Hospital of Parral follow up cases in monthly appointments and attend to complex cases in person.
2.1. Clinical cases on the digital platform
2.1.1. Crossbite
The procedure entails centering dental midlines, matching the upper labial frenulum with the lower one, creating a bite registration with utility wax or silicone putty, removing one of the bite blocks, visualizing the required height of the direct tracks, and creating them in accordance with the diagram, that is to say, mesially higher and with a distal inclination.
Fig. 1MVF 9 years 5 months of treatment

a)

b)
c)
Ask the patient to protrude their mandible to perform a construction bite, centering the upper and lower midlines, creating the bite registration in utility wax or silicone putty, removing one of the registrations, and then preparing the Planas direct tracks in accordance with the Class II schematic, i.e. higher distally and mesially inclined.
Fig. 2ACV 7 years 3 months of treatment

a)

b)
c)
Fig. 3Class II bite II – SN 8 years 3 months of treatment

a)

b)
c)
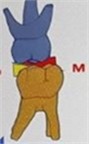
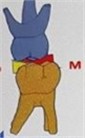
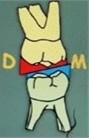
Ask the patient to occlude, matching the upper and lower midlines, make the bite registration in that position with either utility wax or silicone putty, register the height of the crossbite section, and create the direct track in order to correct the crossbite section on the left. This track has a palatal inclination on upper molars and lingual inclination on lower molars, and higher in upper vestibular and lower lingual, according to the chart.
Fig. 4Unilateral left crossbite – GRM 6 years 3 months of treatment

a)

b)

c)
2.2. Law of transversal and saggital developlemt (Pedro Planas)
In vicious mastication, the condylar movement of the BALANCE SIDE produces neural excitation (NE) that, in turn, causes growth of the hemimandible of the balancing side due to displacement. On the WORK SIDE, the neural excitation caused by the contact of the occlusal surfaces stimulates the development of the upper maxillary hemi-arch, i.e. the maxillary on the working side grows due to friction.
Fig. 5Balance side work side
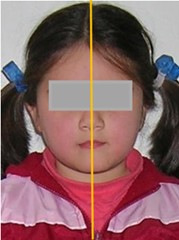
This photograph shows a unilateral left crossbite. In search of balance, the mandible always approaches the maxilla as much as possible. This corresponds to the minimum vertical dimension (working side). In children with posterior unilateral crossbite, mastication is performed on this side, which is evidence for Planas’ law of the minimum vertical dimension [10].
Fig. 6Left crossbite

3. Discussion
The implementation of teleodontology in Chile has meant a leap towards the modernization of oral care, especially after the post-pandemic context of 2020. Applying the knowledge of functional maxillary orthopedics through neuro-occlusal rehabilitation in the teleorthodontics of the Ministry of Health has proven to be an effective measure to approach dental maxillary anomalies in its early stages, crucial for the normal development of the stomatognathic system of children.
3.1. Benefits of teleodontology
Broader access: Teleodontology allows more patients – particularly from rural and hard-to-reach areas – to receive specialized care without the need to travel long distances.
Continuing training: Training primary health care dentists in new digital techniques and tools promotes a more comprehensive and team oriented approach in dental care.
Early intervention: Detecting and treating anomalies in their early stages can help prevent complex problems in the future, improving patients’ quality of life.
Interdisciplinary collaboration: The digital platform that connects odontologists and specialists fosters an environment of continuing learning and multidisciplinary care, which can enrich the practice of dental care.
3.2. Challenges to consider
Technology infrastructure: The effectiveness of teleodontology relies on the availability of technological resources for professionals and patients.
Patients’ acceptance: It is imperative that patients and their families trust and feel comfortable using the digital tools for dental care.
Standards and regulations: It is necessary to establish clear guidelines and regulations that ensure the quality of care and data protection for patients in digital environments.
Education and awareness: Promoting teleodontology requires and education campaign to inform the population about its benefits and how to access it.
4. Results
All of the cases presented satisfactory changes that disrupted the maxillary dental anomaly at its onset during primary dentition, allowing an adequate functioning of the stomatognathic system.
As shown in the crossbites of Fig. 1 and 2, resin was incrementally placed on the upper mesial occlusal surfaces of temporal molars with distal inclination, an adaptation of the ideas of Dr. Planas, in order to move vertical inclination towards the posterior sector, a) initial b) final. Fig. 3 corrects Class II by placing Planas direct tracks on the occlusal surfaces of temporal molars distally and higher with mesial inclination a) initial b) final. In Fig. 4, the placement of direct tracks was prescribed to correct the crossbite of left-side upper and lower molars. As shown in picture number 4, the resin increment was applied from vestibular to palatal in upper molars and from lingual to vestibular in lower molars a) initial b) final. Fig. 5 is an extraoral photograph with unilateral left mastication in which Balancing and Working sides are distinguished.
5. Conclusions
It is demonstrated that odontologists of primary health care in Chile, with the training and guidance of specialist in orthodontics and functional maxillary orthopedics, can identify and/or disrupt dental maxillary anomalies in primary dentition, achieving a functional equilibrium and adjustment of occlusion. Follow-up until permanent dentition to verify long-term stability of the treatment received during primary dentition is recommended [11].
References
-
W. A. Simoes, P. Valerio, and D. Duarte, Functional Orthopedics of the Maxilla: Research and Clinical Excellence. (in Spanish), São Paulo: Napoleão, 2020.
-
W. A. Simoes, Functional Orthopedics of the Jaws Through Neuroocclusal Rehabilitation. (in Spanish), Madrid: Panamericana, 2004.
-
P. Planas, Neuro-Oclusal Rehabilitation. (in Spanish), Medellín: Amolca, 2008.
-
M. Do Amaral Sampaio, Postures and Baby Positions: Specific Level of Prevention. Preventing Malocclusion in Babies. (in Portuguese), São Paulo: Napoleão, 2022.
-
S. Silveira, P. Valerio, and A. J. Machado Júnior, “The law of minimum vertical dimension: evidence for improvement of dental occlusion,” European Journal of Dentistry, Vol. 16, No. 2, pp. 241–250, Oct. 2021, https://doi.org/10.1055/s-0041-1732950
-
J. Zou, M. Meng, C. S. Law, Y. Rao, and X. Zhou, “Common dental diseases in children and malocclusion,” International Journal of Oral Science, Vol. 10, No. 1, pp. 1–7, Mar. 2018, https://doi.org/10.1038/s41368-018-0012-3
-
A. J. I. Garbin, B. Wakayama, T. A. S. Rovida, and C. A. S. Garbin, “Neuroclusal rehabilitation and planas direct tracks in the posterior crossbite treatment,” RGO – Revista Gaúcha de Odontologia, Vol. 65, No. 2, pp. 109–114, Jun. 2017, https://doi.org/10.1590/1981-863720170002000023046
-
M.-A. Cardozo, J.-M. Martínez, N. Molina, and J.-A. Hernández, “Effects of functional maxillary orthopedics on the dimensions of the dental arches in patients with deep bite in primary dentition,” Revista Estomatología, Vol. 24, No. 1, pp. 18–23, Sep. 2017, https://doi.org/10.25100/re.v24i1.5792
-
L. D. ’Onofrio, “Oral dysfunction as a cause of malocclusion,” Orthodontics and Craniofacial Research, Vol. 22, No. S1, pp. 43–48, May 2019, https://doi.org/10.1111/ocr.12277
-
O. Santiago, “Incidence of unilateral chewing in children with primary dentition and early mixed dentition with fibrous and soft foods,” (in Portuguese), Revista da Faculdade de Odontologia de Porto Alegre, Vol. 35, No. 1, pp. 28–31, Aug. 1994.
-
R. R. D. Santos, A. J. Isper Garbin, and C. A. Saliba Garbin, “Early correction of malocclusion using planas direct tracks,” Case Reports in Dentistry, Vol. 2013, p. 395784, Jan. 2013, https://doi.org/10.1155/2013/395784
About this article

The authors have not disclosed any funding.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
The authors declare that they have no conflict of interest.
Participants provided written informed consent prior to the research.
