Abstract
Deep overbite is a malocclusion commonly found in children and difficult to treat, thanks to its instability. Deep overbite is a malocclusion commonly found in children and difficult to treat due to its instability. In deciduous dentition, the most effective treatment is the use of Planas Direct Tracks (PDT), which involves the application of composite resin on the occlusal surfaces of the posterior teeth. Although it is the most effective technique for treating deep bite, it shows a high recurrence rate. To solve this problem, the technique was modified by adding composed resin stops in the lingual face of the upper central incisors. in addition to the traditional tracks on the molars. This study, with the report of 2 clinical cases using the modified PDT, demonstrated that after one year, the treatment was stable and without recurrences, suggesting that the proposed modifications provide more stability than the traditional PDT.
1. Introduction
Deep bite is a common malocclusion in childhood with a prevalence around 18 % to 41.9 % [1-3] and correcting it in the deciduous dentition is challenging due to the high relapse rate. If left untreated, a deep overbite impairs mandibular lateral movements, increasing the functional masticatory Planas angle, making chewing difficult and reducing the expansion promoted by masticatory movements [4-6]. One of the recommended approaches for this type of occlusopathy is the Planas Direct Tracks (PDT) technique, which involves applying composite resin on one or more teeth to promote an immediate change in mandibular posture by increasing the vertical dimension [4]. In this report of 2 cases, we demonstrate a new methodology for applying PDT that provided greater stability in correcting deep bites.
2. Materials and methods
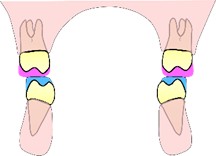
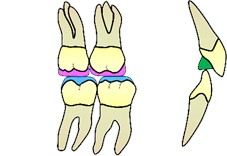
The PDT for deep bite treatment consists mainly of composite resins applied to the occlusal surfaces of the posterior teeth to elevate the bite [4]. Due to the high rate of relapse observed in over 100 cases of deep bite treatment with Planas Direct Tracks (PDT) over a span of more than 20 years, a minor modification was introduced to the track system. This involved adding anterior stops on the palatal surfaces of the upper incisors, also made of composite resin, as illustrated in Fig. 1.
Fig. 1Posterior Planas direct tracks and the anterior stop on the palatal surfaces of the upper incisors (in green)
3. Case 1
A 5-year-old male patient presented for consultation with a history of preference for soft foods and extreme difficulty chewing. On clinical examination, the patient was dolichoprosopic with a deep overbite, characterized by more than 80 % coverage of the lower incisors by the upper incisors, and mild distoclusion. A panoramic radiograph was requested to analyze the bone bases and assess the roots of the incisors to evaluate the feasibility of using bite planes on the teeth in question.
Fig. 2Case 1: initial frontal photo showing the deep bite

Fig. 3Case 1: Installation of the bite block on the palatal surfaces of the upper teeth and the occlusal surfaces of the second molars (occlusal view) and immediate post-installation frontal image


Fig. 4Case 1: frontal view one year after the installation of the modified Planas direct tracks with anterior stops

4. Case 2
A 4-year-old male patient presented for consultation with selective eating habits and a preference for liquids. On clinical examination, the patient was mesoprosopic, with a deep overbite, characterized by more than 100 % coverage of the lower incisors, as well as distoclusion and an accentuated lower Spee curve. The panoramic radiograph showed no technical obstacles to performing bite planes.
Fig. 5Case 2: initial frontal photo showing the deep bite with complete coverage of the lower incisors

Fig. 6Case 2: installation of the bite stop on the palatal surfaces of the upper incisors and the occlusal surfaces of the first molars (occlusal view) and immediate post-installation frontal image


Fig. 7Case 2: Occlusal and frontal photo six months after installation. A significant change in the maxilla, especially in its transverse diameter, can be observed


Fig. 8Case 2: frontal view one and a half years after the installation of the modified Planas direct tracks with anterior stops

5. Discussion
The advantage of treating deep bite with Planas direct tracks lies in the simplicity and biomechanical effectiveness of this method. The direct tracks promote rapid and effective posterior disocclusion, facilitating mandibular repositioning and allowing for functional bite correction. Additionally, by modifying the anterior guide and stimulating condylar growth, they promote more balanced development of the stomatognathic system.
As observed, the anterior stops have different sizes due to the variation in chewing force between the children. The stop with the larger volume was designed to compensate for the greater masticatory load, as seen in patient number 2.
Clinically, the use of Planas tracks can reduce treatment time, as they induce remodeling of the bone bases and relieve pressure on the anterior teeth.
Lastly, this type of intervention minimizes the risk of excessive dental wear and muscular overload by redistributing occlusal forces more homogeneously.
6. Results
In both cases, the insertion of an anterior composite resin stops on the palatal surfaces of the central deciduous incisors, associated with traditional posterior tracks on the molars’ occlusal surfaces, provided greater stability in the medium-term treatment of deep bites. An increase in the transverse growth of the jaws was observed through the appearance of diastemas between incisors and by the intercanine distance, especially the upper one. A more anteriorized position of the mandible has been observed, as indicated by the improvement in the canine keys and the reports from parents of better chewing were observed.
7. Conclusions
Anterior stops on the upper incisors associated with traditional PDT on the molars suggested to be more effective and stable than the conventional technique in treating deep overbite.
References
-
J. P. Sousa and S. A. Sousa, “Prevalence of malocclusion in 7-9-years-old children from Pole 1 of municipal schools in João Pessoa-PB,” (in Portuguese), Revista de Odontologia da UNESP, Vol. 42, No. 2, pp. 117–123, Apr. 2013, https://doi.org/10.1590/s1807-25772013000200009
-
M. A. V. Bittencourt and A. W. Machado, “Prevalence of malocclusion in children between 6 and 10 years of age: a Brazilian panorama,” (in Portuguese), Dental Press Journal of Orthodontics, Vol. 15, No. 6, pp. 113–122, Dec. 2010, https://doi.org/10.1590/s2176-94512010000600015
-
O. G. D. Silva Filho, S. F. Freitas, and A. O. Cavassan, “Prevalence of normal occlusion and malocclusion in the mixed dentition on schoolars in Bauru (São Paulo),” (in Portuguese), Journal of the São Paulo Association of Dental Surgeons, Vol. 43, No. 6, pp. 287–290, 1989.
-
P. Planas, Reabilitação Neuroclusal. 1997.
-
S. Silveira, P. Valerio, and A. J. Machado Júnior, “The law of minimum vertical dimension: evidence for improvement of dental occlusion,” European Journal of Dentistry, Vol. 16, No. 2, pp. 241–250, Oct. 2021, https://doi.org/10.1055/s-0041-1732950
-
M. Limme, “Interception in temporary dentition: chewing and neuro-occlusal rehabilitation,” (in Portuguese), L’Orthodontie Française, Vol. 77, No. 1, pp. 113–135, Oct. 2011, https://doi.org/10.1051/orthodfr/200677113
About this article

The authors have not disclosed any funding.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Rafaella Moura Aragão: conceptualization, data curation, investigation and validation. Pedro Pileggi Vinha: methodology, project administration, supervision and writing-review and editing.
The authors declare that they have no conflict of interest.
All study participants signed authorization for the publication of this case report.
