Abstract
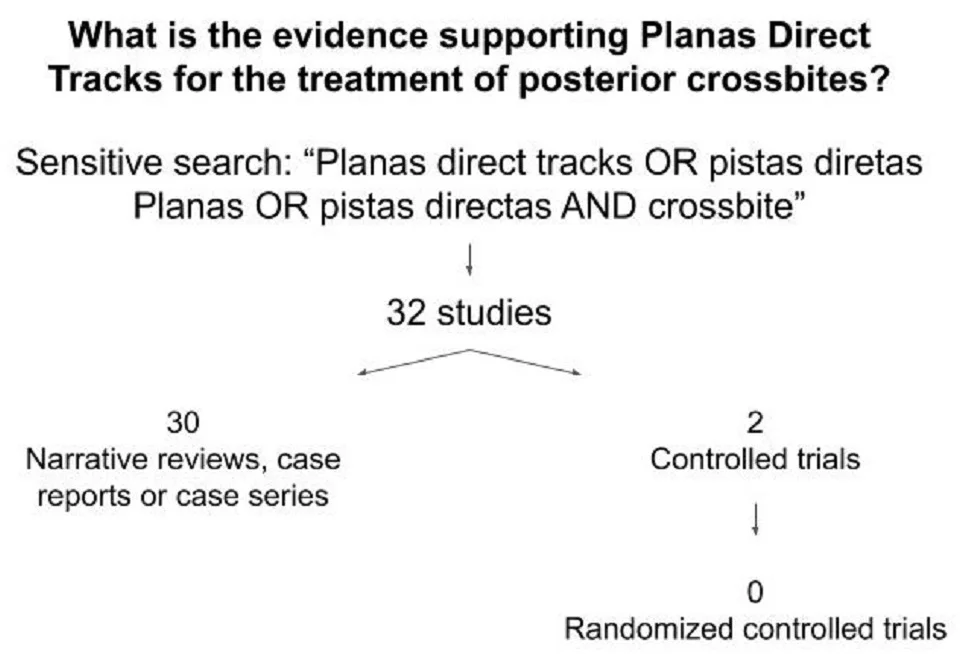
Introduction: Posterior functional crossbite is a common malocclusion in children, with a prevalence between 7.5-24 %. It has an important impact on facial functions, and may cause asymmetries in craniofacial development. Different interventions have been used to correct this malocclusion but there is a lack of studies with methodological rigor that support these interventions. Planas Direct Tracks (PDT) constitute one of such interventions. They seek to reestablish the functional occlusal balance of children through selective grinding, complementing this adjustment with composites. Objective: To present the level of scientific evidence available on PDT to correct posterior crossbites. Method: A sensitive search was carried out in the main databases: Pubmed, BVS Odontology, Cochrane, SciElo and Google academic. The articles were selected, duplications removed and critical evaluation of the literature performed classifying the studies according to the evidence pyramid. The aim is to point out ways to improve the quality of the studies. Results: 32 studies were included. 30 studies were narrative reviews, case reports or case series and two were controlled trials. All studies had important biases. No randomized controlled trial was found. Conclusion: So far, there are no studies, sufficiently rigorous methodology, on Planas direct tracks to correct functional crossbites.
Highlights
- What did I want to find out? Randomized clinical trials to correct crossbites.
- What did I do? A sensitive search strategy in the main databases with free terms "Planas direct tracks or pistas diretas Planas or pistas directas and crossbite".
- What did I find? 32 studies. 30 were narrative reviews, case reports or case series. Two were controlled trials. No randomized controlled trial was found.
- Gaps in the evidence were pointed out in order to collaborate with future research.
1. Introduction
Posterior functional crossbite is characterized by an abnormal buccal, labial or lingual relationship of one or more posterior teeth when these are occluded, with top back teeth biting down inside the bottom back teeth. It is a common malocclusion that presents with maxillary atresy with mandible postural deviation, midline deviation and, frequently, condyle dislocation and asymmetric muscular activity in both sides [1-2]. If uncorrected, it can lead to facial asymmetry [3]. In addition, it has also been associated with sleep breathing disorders in children [4].
Crossbite prevalence in children varies from 7,5 % to 24 % in the deciduous and mixed dentition [5-11]. The studies show that self-correction is seldon [5-6, 12]. Therefore, many interventions have been suggested and are used in daily practice. Most of them are fixed or removal braces [13].
Randomized Clinical Trials (RCTs) are robust studies to evaluate interventions. The patients are randomly allocated to two comparison groups and after follow-up the outcomes in each group are evaluated. Care in the design, conduct and results analysis are crucial. Sample size calculation, allocation concealment, blind outcome evaluation, and intention-to-treat analysis bring the methodological rigor necessary to conclude whether a given intervention is effective or not [14-15].
Randomization equally divides patients between comparison groups in terms of prognostic determinants. There is no researcher control over the decision to assign a patient to one or another group. Patients do not participate in this decision as well. For example, a sequence of random numbers in a computer program is an adequate form of randomization.
RCTs are important to avoid biases (systematic errors) when comparing treatments. Patients are similar in all prognostic determinants (age, crossbite characteristics, disease severity and any other possible confounder - predictable or not) differing only in what is being tested (with or without treatment, for example) [14].
Systematic reviews aim to search for randomized clinical trials on interventions in the health area. If the studies are homogeneous, the results can be summed up on a meta-analysis. Cochrane Systematic review on crossbite treatments, updated in 2021, concluded that quad-helix and expansion plates are more beneficial than no treatment for correcting posterior crossbites in children aged 7-11 years old [13]. “The remaining evidence was insufficient to draw any robust conclusions for the efficacy of posterior crossbite correction” according to such systematic review [13]. Planas direct tracks is one of these interventions, created by Pedro Planas and named by Wilma Simões, and it has been routinely used in practice since the 70 s [16-17] Fig. 1.
Fig. 1Planas direct tracks

a) Initial

b) Planas direct tracks

c) Follow up – 1 year
The treatment consists of reestablishing occlusal balance through selective grinding complemented with the application of composites. It starts by eliminating interferences between the centric occlusion position and maximum intercuspation, in general, in the canine area. Such interferences shift the mandible to the crossed side. After that, occlusal adjustment seeks to equalize the vertical dimensions of both sides, within the child's tolerance limit. Finally, the contacts are complemented with composites.
Planas recommends keeping a minimum vertical dimension on the non-crossed side until the mandibular deviation is corrected [16]. After that, the vertical dimension of both sides can be equalized.
The final objective is to obtain balanced contacts both in the position of maximum intercuspation, coinciding with centric occlusion, and also in left and right lateral movements, without shift or direction changes [18].It is a simple intervention, performed directly in the mouth, requiring no adherence to the treatment. In addition, it can be used earlier, around 4 years of age, with an important positive impact on the child's growth and development. Nevertheless, despite the routine use in daily practice, there are few studies available on this intervention.
The objective of this article is to determine the level of scientific evidence available to support this intervention in the treatment of posterior functional crossbite.
2. Method
2.1. Inclusion criteria
All studies about Planas direct tracks intervention in the treatment of posterior crossbites in children.
2.2. Search strategy
The following search strategy with free terms was developed and conducted until may of 2022, on pubmed and adapted for the following databases: lilacs; BBO (Brazilian Bibliography of Dentistry); SciELO, The Cochrane library and Google scholar: “Planas direct tracks or pistas diretas Planas or pista direta Planas or pistas directas de Planas and crossbite”. The decision not to refine the search was based on the expectation to find few specific studies. The objective was to make a sensitive search of results.
2.3. Cross-checking references
References from original papers and review articles were checked.
2.4. Method of the review
The eligibility of all reports identified were assessed by titles and abstracts. After screening the studies, the inclusion criteria were applied. All studies related to the Planas direct tracks intervention and treatment of functional crossbites were included.
The studies were classified according to the type of study [15, 19]:
1. In vitro.
2. Animal research.
3. Expert opinion (including narrative review).
4. Case report or Case series.
5. Case-control.
6. Cohort.
7. Randomized controlled trial.
8. Systematic review.
If randomized controlled trials were found, four main quality aspects would be considered on the methodological judgements of the trials:
1. Allocation concealment.
2. Blind outcome assessment.
3. Completeness of follow up.
4. Intention-to-treat analysis.
Studies would be classified as low, moderate or high risk of bias according to the Cochrane Handbook for Systematic review [20]..The main results on the quality of the studies would be summarized.
3. Results
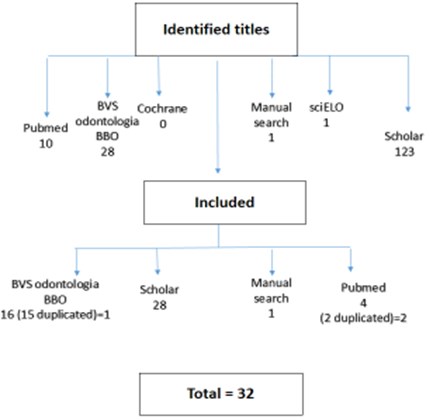
The results are described in Fig. 2.
163 studies were potentially eligible, but 32 were included [21-52].30 studies were narrative reviews, case report or case series and two studies were controlled trials.
In the first controlled trial [21] the sample consisted of 20 children, 4 to 6 years old, divided into two groups, paired up according to age and gender. The group test consisted of 10 functional posterior crossbite patients treated with PDT built only in canines and molars and the control group consisted of 10 normal occlusion children. These direct tracks were kept for four months and after that were removed. The primary outcome was the intercanine and intermolar distance. The author concluded that the treatment with PDT was able to give back the normal dimensions of the deciduous arch. The uncrossing of the bite was not considered as an outcome.
The second controlled trial [22] included 11 children, 6-9 years old. All children had functional posterior crossbite. The children were aleatory divided into two groups: Group 1: 5 children treated with PDT. Group 2: 6 children treated with Quad helix appliance. The author described sample size calculation, signed consent form, ethics committee approval, case severity defined as mild or moderate, clear exclusion criteria, such as digital sucking habits. The randomization criteria were not described and the proposed outcome was transverse changes in the maxilla. The results could not be evaluated due to the withdrawal of 6 patients (more than 50 % of the sample).
Fig. 2Fluxogram of the included studies
Both controlled trials had a small number of patients, asymmetric comparison groups, without randomization and did not have bite uncrossing as a primary outcome. So, it is not possible to conclude effectiveness or efficacy of the direct tracks on crossbite treatment based on these two studies.
The main case series study [23] included 43 children 3-6 years old with functional posterior crossbite. All children were treated with PDT and were followed for 91 days. The results indicated 79 % of success at uncrossing the bites. The author reported that 79,4 % of the children had some sucking habit at the beginning of the study and 94,1 % had this deleterious habit ceased at the end of the study. In fact, it is an important confounder that can have changed the results. If there was a comparison group with randomization, uncontrolled factors would be aleatory divided into the two groups, decreasing the chance of bias. Although the study can suggest some efficacy, this study does not have a comparison group, nor randomization. So, it is not possible to conclude effectiveness or efficacy of the direct tracks on crossbite treatment based on this study.
No randomized controlled trial was found.
4. Discussion
This search did not find any RCT about Planas Direct Tracks. The main biases of the included studies are the lack of standardization of outcomes, absence of a control group, absence of randomization, absence of sample size calculation and lack of control for confounding factors.
Other important methodological flaws were found. Functional crossbite characteristics (ex: severity, number of teeth involved) and patient age at the time of intervention were not described. Relevant outcomes were not adequately defined and/or reported, such as correction of midline deviations and the definition of bite uncrossing. The latter is particularly important in the context that edge-to-edge bites in teeth with direct tracks may confound this assessment. Specific criteria for the outcome of bite uncrossing should be prespecified.
Detailed description of the method of using the Planas Direct Tracks should also be published to standardize the procedure from selective grinding to composites and occlusion readjustment. These are important factors to be standardized. Confounders such as deleterious habits and respiratory disorders also need to be controlled.
So far, there are no RCTs with a rigorous methodology on Planas direct tracks to correct functional crossbites.
Absence of evidence does not mean no effect in crossbite treatment with Planas direct tracks, but the absence of well-designed studies. Healthcare treatment decisions should be based on available evidence, professional experience and patient consent [19].
Jaw Functional Orthopedics is a relatively recent specialty in Brazil (2001) and it is extremely important that studies are conducted following international criteria of high quality scientific evidence, in order to contribute to the growth of this important specialty.
5. Implications for future research
From an evidence-based point of view, randomized controlled trials with rigorous methodology should be adopted to elucidate such intervention:
1. Sample of adequate size based on power calculation; adequate sequence of randomisation with allocation concealment (for example sequence of random numbers); blind outcome assessment or, if it not possible, independent assessment (for example, researcher who is not involved in the trial); completeness of follow-up. If there are dropouts, the analysis should be done by intention to treat, and the data described by the author [15].
2. The diagnostic criteria for crossbite must be standardized, including crossbite characteristics such as number of crossbite teeth, severity and age at the time of intervention.
3. Potential confounders of results such as deleterious habits should be controlled or these patients should be excluded.
4. The primary outcome must be crossbite uncrossed. Outcomes should be standardized, including which criteria are considered to assess bite uncrossing, amount of maxillary and mandibular growth, stability of correction, follow up, costs, tolerability and the measures to assess these outcomes.
5. Validity and reliability of measurement instruments frequently used such as intermolar and intercanine distance measured on plaster casts or cone beam tomography, Planas gnathostatic models or Camper plan protractor (or positioner) are required.
6. The control group can be a non-intervention group until the end of follow-up, being treated later. Different interventions can also be compared.
7. Interactions between crossbite and respiratory disorders or swallow disorders can be researched together with another professional in a translational approach within randomized clinical trials.
8. The quality of RCTs can improve if the guideline CONSORT is used [52].
6. Conclusions
The current level of available evidence for the use of Planas direct tracks to correct functional crossbite is case series.
Given that there are not randomized controlled trials to support this intervention, recommendations for clinical practice cannot be made based only on the results of the current available studies. Randomized controlled trials are needed to elucidate this intervention on crossbite treatment.
References
-
B. Thilander and K. Bjerklin, “Posterior crossbite and temporomandibular disorders (TMDs): need for orthodontic treatment?,” The European Journal of Orthodontics, Vol. 34, No. 6, pp. 667–673, Dec. 2012, https://doi.org/10.1093/ejo/cjr095
-
K. L. Hesse, J. Årtun, D. R. Joondeph, and D. B. Kennedy, “Changes in condylar position and occlusion associated with maxillary expansion for correction of functional unilateral posterior crossbite,” American Journal of Orthodontics and Dentofacial Orthopedics, Vol. 111, No. 4, pp. 410–418, Apr. 1997, https://doi.org/10.1016/s0889-5406(97)80023-6
-
K. Behlfelt, S. Linder-Aronson, J. Mcwilliam, P. Neander, and J. Laage-Hellman, “Dentition in children with enlarged tonsils compared to control children,” European Journal of Orthodontics, Vol. 11, No. 4, pp. 416–429, Nov. 1989, https://doi.org/10.1093/oxfordjournals.ejo.a036014
-
G. Kutin and R. R. Hawes, “Posterior cross-bites in the deciduous and mixed dentitions,” American Journal of Orthodontics, Vol. 56, No. 5, pp. 491–504, Nov. 1969, https://doi.org/10.1016/0002-9416(69)90210-3
-
K. Heikinheimo, K. Salmi, and S. Myllarniemi, “Long term evaluation of orthodontic diagnoses made at the ages of 7 and 10 years,” The European Journal of Orthodontics, Vol. 9, No. 2, pp. 151–159, May 1987, https://doi.org/10.1093/ejo/9.2.151
-
A. Hannuksela and A. Väänänen, “Predisposing factors for malocclusion in 7-year-old children; with special reference to atopic diseases,” American Journal of Orthodontics and Dentofacial Orthopedics, Vol. 92, No. 4, pp. 299–303, Oct. 1987, https://doi.org/10.1016/0889-5406(87)90330-1
-
O. G. D. Silva Filho, S. F. Freitas, and A. O. Cavassan, “The prevalence of normal occlusion and malocclusion in school children from Bauru,” (in Portuguese), Revista da Associação Paulista de Cirurgiões Dentistas, Vol. 43, No. 6, pp. 287–90, Dec. 1989.
-
E. S. Moraes, C. C. Lira, M. Ely, Thomaz E. B., and A. M. G. Valença, “Prevalence of openbite and crossbite in deciduous dentition,” (in Portuguese), Revista Brasileira de. Ciências da. Saúde, Vol. 5, No. 1, pp. 23–30, Jan. 2001.
-
O. G. Silva Filho, P. R. Baleirine E. Silva, M. V. N. N. Rego, and L. Capelozza Filho, “Epidemiology of the posterior crossbite in the primary dentition,” (in Portuguese), Journal Brasileiro de Odontopediatria and Odontologia do Bebê,, pp. 61–68, 2003.
-
F. R. Carvalho, D. A. Lentini-Oliveira, G. M. M. Carvalho, L. B. F. Prado, G. F. Prado, and L. B. C. Carvalho, “Sleep-disordered breathing and orthodontic variables in children-Pilot study,” International Journal of Pediatric Otorhinolaryngology, Vol. 78, No. 11, pp. 1965–1969, Nov. 2014, https://doi.org/10.1016/j.ijporl.2014.08.040
-
B. Thilander, S. Wahlund, and B. Lennartsson, “The effect of early interceptive treatment in children with posterior cross-bite,” The European Journal of Orthodontics, Vol. 6, No. 1, pp. 25–34, Jan. 1984, https://doi.org/10.1093/ejo/6.1.25
-
A. Ugolini, P. Agostino, A. Silvestrini-Biavati, J. E. Harrison, and K. B. Batista, “Orthodontic treatment for posterior crossbites,” Cochrane Database of Systematic Reviews, Vol. 2021, No. 12, Dec. 2021, https://doi.org/10.1002/14651858.cd000979.pub3
-
R. H. Fletcher, S. W. Fletcher, and E. H. Wagner, Epidemiologia clínica: elementos essenciais. Artmed, 1996.
-
D. C. Slawson, “How to Read a Paper: The Basics of Evidence Based Medicine, by Trisha Greenhalgh,” BMJ, Vol. 315, No. 7112, pp. 891–891, Oct. 1997, https://doi.org/10.1136/bmj.315.7112.891
-
P. Planas, Reabilitação Neuro-Oclusal. MDSI, 1988.
-
W. A. Simões, Ortopedia Funcional dos Maxilares vista através da Reabilitação Neuro-Oclusal. Santos, 1985.
-
Oliveira and D. A. L., “Ortopedia funcional na odontopediatria,” in Ortodontia, Ortopedia Funcional, 2002.
-
N. A. Atallah. “Caminhos do Pensamento. Medicina Baseada em Evidências”, http://www.centrocochranedobrasil.org.br/apl/artigos/artigo_516.pdf
-
J. P. T. Higgins, D. G. Altman, and J. A. C. Sterne, “Assessing risk of bias in included studies,” in Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0, 2017.
-
A. C. Chibinski and G. Czlusniak, “Evaluation of treatment for functional posterior crossbite of the deciduous dentition using Planas’ direct tracks,” Indian Journal of Dental Research, Vol. 22, No. 5, p. 654, 2011, https://doi.org/10.4103/0970-9290.93451
-
L. C. Moreno Páez, Y. A. Ramírez Vega, D. M. Rozo Salinas, Especialista En Ortodoncia Y. Ortopedia Maxilar, and Especialización, “Determination of transversal changes in maxilla after the treatment with Direct Flat Tracks vs. Quad Hélix. Pilot Study,” (in Portuguese), Journal Odontológico Colegial, Vol. 11, No. 22, pp. 15–21, 2018.
-
A. J. I. Garbin, B. Wakayama, T. A. S. Rovida, and C. A. S. Garbin, “Neuroclusal rehabilitation and planas direct tracks in the posterior crossbite treatment,” RGO – Revista Gaúcha de Odontologia, Vol. 65, No. 2, pp. 109–114, Jun. 2017, https://doi.org/10.1590/1981-863720170002000023046
-
W. A. Simões, “Selective grinding and Planas’ direct tracks as a source of prevention,” Journal of Pedodontic, Vol. 5, No. 4, pp. 298–314, 1981.
-
M. R. Brandão, “Pista direta Planas na correção da mordida cruzada posterior,” Revista da APCD, Vol. 49, pp. 127–129, 1995.
-
Oliveira and D. A. L., “Funcional crossbites in children: Planas direct tracks,” (in Portuguese), Ortodontia, Vol. 30, No. 1, pp. 92–100, 1997.
-
M. N. Gribel, “Planas direct tracks in the treatment of unilateral crossbite with mandibular postural deviation,” (in Portuguese), Revista Dental Press de Ortodontia e Ortopedia Maxilar, Vol. 4, No. 5, pp. 47–54, 1999.
-
H. A. Oliveira and G. Ortellado, “Planas Direct Tracks for posterior crossbite correction,” (in Portuguese), Jornal brasileiro de ortodontia e ortopedia facial, Vol. 6, No. 31, pp. 15–19, 2001.
-
M. N. Gribel, “Planas direct tracks in the early treatment of unilateral crossbite with mandibular postural deviation. Why worry so soon?.,” Orthodontics, Vol. 3, No. 3, pp. 239–249, 2002.
-
Ramirez-Yañez Go, “Planas direct tracks for early crossbite correction,” Journal of Clinical Orthodontics: JCO, Vol. 37, No. 6, pp. 294–8, Jun. 2003.
-
A. C. Chibinski, Czlusniak G. D., and Melo M. D., “Planas direct tracks: orthopedic treatment to correct functional crossbite,” (in Portuguese), Revista Clínica de Ortodontia Dental Press, Vol. 4, No. 3, pp. 64–72, 2005.
-
G. P. Neto, R. M. Puppin-Rontani, and R. C. M. R. Garcia, “Changes in the masticatory cycle after treatment of posterior crossbite in children aged 4 to 5 years,” American Journal of Orthodontics and Dentofacial Orthopedics, Vol. 131, No. 4, pp. 464–472, Apr. 2007, https://doi.org/10.1016/j.ajodo.2005.06.030
-
M. R. Padilla, L. R. Tello, and J. A. Hernández, “Early approach of the transversal malocclusions, diagnosis and treatment: literature review,” (in Portuguese), Revista Estomatologia, Vol. 17, No. 1, pp. 30–37, 2009.
-
R. R. Santos, “Ortodontics in public health: Planas Direct Tracks as an alternative treatment for earlier correction of malocclusion,” (in Portuguese), Ph.D. Thesis, Faculdade de Odontologia, Universidade Estadual Paulista, 2011.
-
R. R. D. Santos, A. J. Isper Garbin, and C. A. Saliba Garbin, “Early correction of malocclusion using planas direct tracks,” Case Reports in Dentistry, Vol. 2013, pp. 1–4, 2013, https://doi.org/10.1155/2013/395784
-
Artenio Jose Isper Garbin, Bruno Wakayama, Renata Reis Dos Santos, Tania Adas Saliba Rovida, and Clea Adas Saliba Garbin, “Pistas directas planas para el tratamiento de la mordida cruzada posterior,” Revista Cubana de Estomatología, Vol. 51, No. 1, pp. 52–59, May 2014.
-
A. J. I. Garbin, B. Wakayama, T. A. S. Rovida, and C. A. S. Garbin, “A utilização da Pista Direta de Planas no tratamento precoce da mordida cruzada posterior: relato de caso,” Archives of Health Investigation, Vol. 5, No. 4, Sep. 2016, https://doi.org/10.21270/archi.v5i4.1326
-
I. D. Piñal Luna, P. Molinero Mourelle, L. Torres Moreta, and B. Bartolomé Villar, “Early treatment of unilateral posterior cross bite in the child patient. Literature review,” (in Portuguese), Revisión bibliográfica, Vol. 13, No. 1, pp. 41–48, 2016.
-
Rogério de Mendonça M., Gonçales Verri Ac, Pimenta Martins L., and Aparecido Cuoghi O., “Case report of posterior crossbite: Description of an effective treatment protocol,” Compendium of Continuing Education in Dentistry, Vol. 37, No. 8, Sep. 2016.
-
Jose Isper Garbin Artenio, G. Peres, T. A. Saliba, Bruno Wakayama, and C. A. Garbin, “Neuro-occlusal rehabilitation by the Planas direct tracks method: case report,” Annali di Stomatologia, 2018.
-
P. A. Vedoato, “Planas Directs Tracks – A intervention in children with crossbite in the context dental public,” (in Portuguese), Bachelor thesis, Faculdade de Odontologia de Araçatuba, Universidade Estadual Paulista, 2018.
-
G. P. Teruel, “Neuroclusal rehabilitation by the Direct Direct Paths method,” (in Portuguese), Master thesis, Universidade Estadual Paulista, 2018.
-
M. I. D.Bérgamo, “Neurocclusal Rehabilitation and Public Health – An available resource for the early intervention of malocclusion,” (in Portuguese), Bachelor thesis, Faculdade de Odontologia de Araçatuba, Universidade Estadual Paulista, Araçatuba, 2018.
-
M. de Freitas Oliveira, K. Pantoja de Araújo, K. Pantoja de Araújo, M. I. Monteiro Buelau, and P. John Buelau, “Reabilitação neuroclusal em paciente odontopediátrico com mordida cruzada posterior unilateral relato de caso clínico,” RFO UPF, pp. 31–37, 2019.
-
N. Mora Zuluaga, J. A. Hernández, and C. Rodriguez, “Treatment of unilateral posterior cross-bite in primary and mixed early dentition: Case series,” (in Portuguese), Revista Estomatología, Vol. 27, No. 1, pp. 43–55, Dec. 2019, https://doi.org/10.25100/re.v27i1.8407
-
A. Garbin et al., “Early intervention of crossbite by planas direct tracks: follow up report after seven years.,” Revista Ciencias de la Salud, Vol. 18, No. 2, pp. 119–128, 2020.
-
G. Murakami, “Performance of Planas Direct Tracks during the treatment of functional crossbite,” Bachelor thesis, Faculdade de Odontologia de Araçatuba, Universidade Estadual Paulista, Araçatuba, 2020.
-
M. Del Carmen Prieto, A. C. Medina, and J. E. Mata, “Posterior buccal crossbite correction in the primary dentition. Report of two cases,” Revista de Odontopediatria Latinoamericana, Vol. 6, No. 2, pp. 126–133, Jun. 2020.
-
A. J. I. Garbin et al., “Neuroclusal rehabilitation and Planas direct tracks in the treatment of functional crossbite in children: case report,” (in Portuguese), RSBO: Revista Sul-Brasileira de Odontologia, Vol. 18, No. 2, pp. 382–389, 2021.
-
Silva and M. I. F., “Utilização de rampas de compósito em tratamentos de ortodontia interceptiva: revisão sistemática,” Universidade Fernando Pessoa, Faculdade de Ciências da Saúde, Porto, 2021.
-
R. C. A. Gondim, K. D. P. Pereira, M. M. Gondim, M. P. B. T. Júnior, and P. D. Rebouças, “A utilização de pistas diretas planas no tratamento da mordida cruzada funcional: uma revisão de literatura,” Brazilian Journal of Development, Vol. 7, No. 5, pp. 53541–53557, May 2021, https://doi.org/10.34117/bjdv7n5-656
-
A. P. S. Pereira, G. B. R. Prestes, N. Sarmento, A. L. T. Dutra, V. S. L. Braga, and C. I. O. Carvalhal, “Pista direta planas para tratamento de mordida cruzada anterior funcional relato de caso,” Ortho Science: Orthodontic Science and Practice, pp. 56–61, 2021.
-
D. Moher et al., “Consort 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials,” BMJ, Vol. 340, No. mar23 1, pp. c869–c869, Mar. 2010, https://doi.org/10.1136/bmj.c869
About this article

The authors have not disclosed any funding.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
The research met all applicable standards for the ethics of experimentation. Participants provided written informed consent prior to the study.
