Abstract
Hospitals generate a high amount of carbon dioxide emissions into the atmosphere compared with residential and commercial buildings. Therefore, it is necessary to quantify and identify the CO2 emissions derived from energy consumption in hospitals, studying their relationship with functional variables. The aim of this article is to analyze the CO2 emissions derived from the hospital energy consumption. In Spain, 14 hospitals were analyzed, studying the built surface area and the number of beds in the period 2010-2014. The results showed that in a hospital, the average annual CO2 emissions divided by built surface area is around 0.10 Ton per m2, and the annual CO2 emissions divided by number of beds is around 13 Ton per bed. These ratios will make it possible to benchmark hospital management and set targets for limiting emissions into the atmosphere.
Highlights
- CO2 emissions derived from the hospital energy consumption in Spain was analyzed.
- 14 Spanish hospitals were studied in the period 2010-2014.
- The average annual CO2 emissions divided by built surface area was 0.10 ton per m2.
- The average annual CO2 emissions divided by number of beds was 13 ton per bed.
1. Introduction
Hospitals are one of the buildings with higher CO2 emissions into the atmosphere, compared with residential and commercial buildings, due to their continuous and complex operation [1]. Mitigating climate change requires management strategies that reduce greenhouse gas emissions [2]. It is estimated that an increase in greenhouse gas emissions into the atmosphere by human action may lead to an increase in global terrestrial temperature. Hospitals need an acceptable facilities design, a high construction quality and an effectiveness of the maintenance [3]. Hospitals have a complex energy systems and conventional energy sources, i.e. heating oil, natural gas and electricity [4]. Given the importance of the environmental impacts associated with greenhouse gas emissions from the energy consumption of a hospital, it is interesting to deepen the quantitative estimation of its CO2 emissions [5].
The greenhouse gas emissions in hospitals varies depending on the type and year of construction, the mode of operation, their location and the local climate [6]. The volume of modern healthcare facilities, with a high number of activities and processes, has an important carbon footprint; this impact must be managed by authorities and companies, from an economic point of view, through energy efficiency [7], reduced emissions and use of a sustainable value chain [8].
In the UK, hospitals generate more than 18 billion tonnes of CO2 per year, representing 25 % of total public sector emissions [9]. Hospital activities are estimated to account for between 3 % and 8 % of the climate change footprint in developed countries such as England or United States of America [10].
Bakaimis y Papanikolaou (2017) estimated a 45 % reduction in the electricity consumption of a Greek hospital resulting from the implementation of energy policies [11]. They proposed an investment in photovoltaic panels and the change from current lighting technology to LEDs.
Jiang et al. (2012) conducted an energy audit of 22 tertiary hospitals in Tianjin [12]. They calculated that the annual average carbon emissions was between 131 and 157 kg CO2/m2. In addition, Blass et al. (2015) realized a literature review on environmental sustainability, performance measurement, and healthcare operations management in hospitals [13]. In other hand, Sung et al. (2011) analyzed the energy and carbon dioxide emission caused by power consumption [14] and Gordillo-Orquera et al. (2018) analyzed the electrical load predictability of a large hospital and that of its associated primary care center [15].
Wang et al. (2016) conducted a survey at the Beijing Municipal Health Bureau in order to assess the energy conservation efforts [16]. The results showed that the economic incentives, appropriate technology, enforceable laws and regulations have become the most significant obstacles to the improvement of energy efficiency.
Shi et al. (2019) analyzed the impact of hospital energy saving measures on hospital energy consumption through a survey data of 4 hospitals in Xi'an [17]. The results showed that energy consumption management in hospitals have a significant impact on the CO2 emissions. Nevertheless, in Spain, the CO2 emissions from energy consumption in hospitals have not been enough analyzed, although studies of others healthcare centers have been carried out [18]. Knowing the average values of greenhouse gas emissions allows to get reference limits useful for controlling the environmental efficiency of a hospital.
The aim of this paper is to analyze and quantify the CO2 emissions from energy consumption in Spanish hospitals, according their built surface area and number of beds.
2. Methodology
A quantitative study was carried out in 14 hospitals located in Spain. The data analyzed were obtained from European Union standard EMAS [19] between 2010 and 2014. EMAS recognizes organizations that have implemented a system of Environmental Management.
Two variables were studied: the built surface area of a hospital and its number of beds. Conversion factors were used to calculate the equivalent amount of renewable primary energy, non-renewable primary energy and total primary energy from the final amount of energy consumed by a given thermal installation in a building.
3. Results
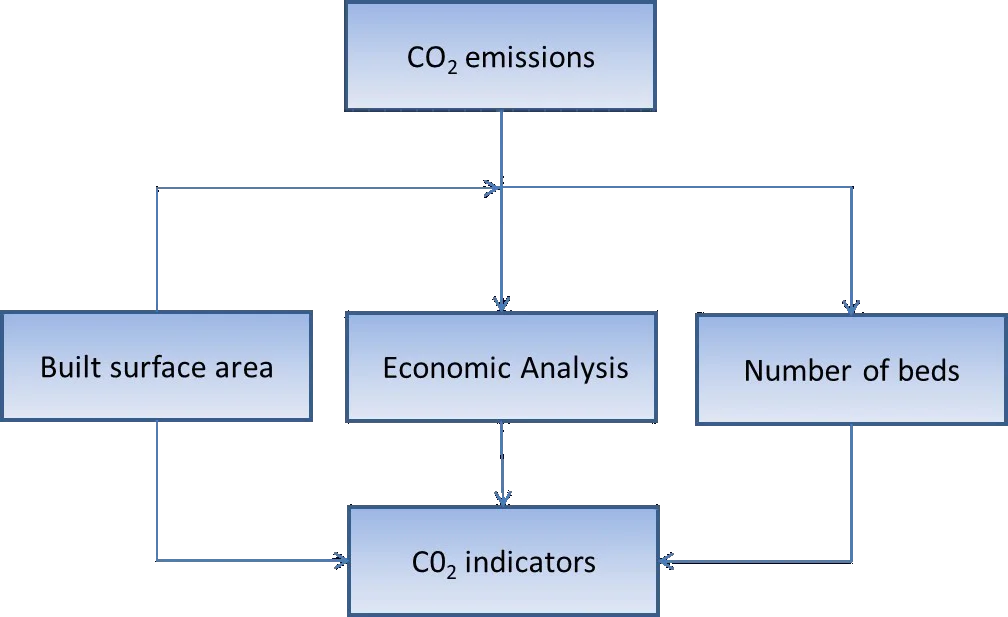
The correlation between the average CO2 emissions per year and the built surface area and the number of beds is presented.
Fig. 1 shows the statistical correlation between the built surface area and the average annual CO2 emissions, expressed in Ton/m2. A high correlation ( 0.8855) was observed between the variables average annual CO2 emissions and built surface area.
Fig. 1Relationship between average annual CO2 emissions and hospital built surface area
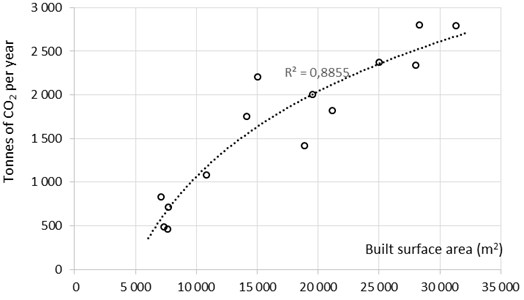
Fig. 2 shows average annual CO2 emissions per built surface area of the hospital, expressed in Ton/m2.
The average annual CO2 emissions divided by built surface area is 0.096 Ton CO2/m2 (std = 0.0221).
The relationship between average annual CO2 emissions (in Tonnes of CO2) and number of hospital beds are presented in Fig. 3. The correlation coefficient (0.7738) is the lowest than the indicator annual CO2 emissions per built surface area indicator.
The average annual CO2 emissions per bed (Ton CO2/bed) is shown in Fig. 4.
Fig. 2Average annual CO2 emissions per built surface area of the hospital
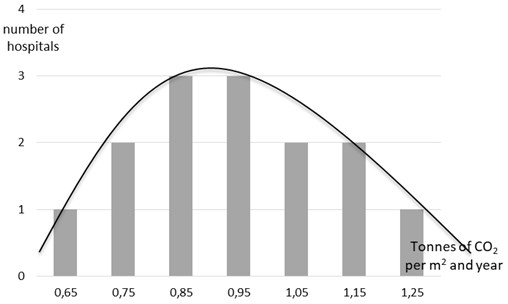
Fig. 3Relationship between average annual CO2 emissions and number of hospital beds
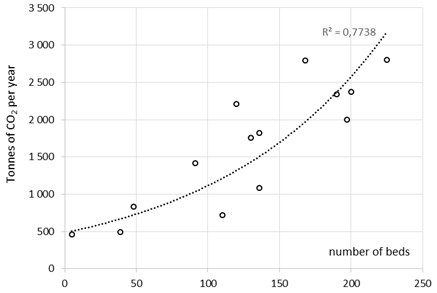
Fig. 4Average annual CO2 emissions per bed
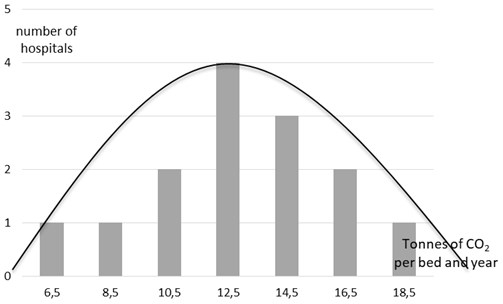
The average annual CO2 emissions according to the number of hospitals beds is 12.97 Ton CO2/bed (std = 3.349).
4. Discussion
The results show that the annual CO2 emissions of a hospital due to its energy consumption are directly related to its built surface area and number of beds.
An adequate hospital maintenance policy must take into account and adequately control the CO2 emissions derived from energy consumption [20]. In addition, an adequate energy savings will allow a proportional reduction in the hospital's CO2 emissions. It is advisable to carry out periodic audits to determine the annual CO2 emissions in each hospital and the appropriate savings measures [21].
The facades and roofs of hospital buildings can increase CO2 emissions from energy consumption; therefore, the materials that make them up must be chosen appropriately [22].
The legislation should incorporate a maximum limit on emissions of CO2 and other greenhouse gases in the construction phase of buildings. The embedded CO2 is increasingly becoming a significant part of the global carbon load of buildings [23]. This would favor the choice of materials with less environmental impact in the design process [24]. The use of renewable energies is an appropriate strategy to combat global warming, reducing CO2 emissions and energy dependency [25]. Therefore, it is also very important to optimize the design of healthcare buildings [26].
The results of this research can serve as a starting point for the development of indicators to quantify the exact consumption of CO2 emissions in hospitals; although none of the CO2 saving measures may alter health and comfort of users [27]. It is also possible to establish quotas for energy consumption and gas emissions in hospital buildings, as proposed by Li et al. [28].
It may be of interest to repeat research in other countries for to establish a comparison about the environmental efficiency. Future researches would be focused in to correlate the building quality with its CO2 atmosphere emissions and to perform simulations of energy behavior [29].
5. Conclusions
In this research, the annual CO2 emissions as a function of the number of beds and the built surface area of a hospital was studied. The correlation found between the CO2 emissions of a hospital with its built surface area was 12.61 % higher than with its number of beds. The results showed that the average annual CO2 emissions from energy consumption in Spanish hospitals divided by built surface area in a hospital is 0.10 Ton/m2. Average annual CO2 emissions divided by number of bed of Spanish hospitals is 13 Ton/bed.
During this study, it was observed that it is necessary a greater implication of the Spanish managers, the sensitization in energetic saving of the users, and an adequate policy of energetic improvement of the healthcare infrastructures to decrease the emissions of gases with greenhouse effect to the atmosphere.
Hospitals should implement an environmental management system focused on minimizing carbon dioxide emissions into the atmosphere. Quantifying a hospital’s CO2 emissions allows hospital managers to make benchmarking with other hospitals and analyze their energy management policy. The path to efficient hospitals requires the incorporation of efficient energy production and storage systems, the control of incorporated energy from the design of building processes and elements, and the adoption of appropriate durability and rehabilitation strategies.
References
-
Vourdoubas J. Energy consumption and carbon emissions in Venizelio hospital in Crete, Greece: can it be carbon neutral? Journal of Engineering, Vol. 6, Issue 1, 2018, p. 19-27.
-
Vidal R., Moliner E., Pikula A., Mena Nieto A., Ortega A. Comparison of the carbon footprint of different patient diets in a Spanish hospital. Journal of Health Services Research and Policy, Vol. 20, Issue 1, 2015, p. 39-44.
-
Fa Li J., Liying L. Requirements for outdoor air in hospital wards in China. Science and Technology for the Built Environment, Vol. 24, Issue 10, 2018, p. 1150-1155.
-
Vourdoubas J. Creation of zero CO2 emissions hospitals due to energy use: a case study in Crete-Greece. Journal of Engineering and Architecture, Vol. 3, Issue 2, 2015, p. 79-86.
-
Brown L. H., Buettner P. G., Canyon D. V. The energy burden and environmental impact of health services. American Journal of Public Health, Vol. 102, Issue 12, 2012, p. 76-82.
-
García Sanz Calcedo J., Gomez Chaparro M., Sanchez Barroso G. Electrical and thermal energy in private hospitals: consumption indicators focused on healthcare activity. Sustainable Cities and Society, Vol. 47, 2019, p. 101482.
-
Kolokotsa D., Tsoutsos T., Papantoniou S. Energy conservation techniques for hospital buildings. Advances in Building Energy Research, Vol. 6, Issue 1, 2012, p. 159-172.
-
Bilec M. M., Ries R. J., Needy K. L., Gokhan M., et al. Analysis of the design process of green children’s hospitals: focus on process modeling and lessons learned. Journal of Green Building, Vol. 4, Issue 1, 2009, p. 121-134.
-
Saving carbon, improving health: NHS carbon reduction strategy for England. National Health Service, Cambridge, 2009.
-
Chung J., Meltzer D. O. Estimate of the carbon footprint of the US health care sector. Journal of the American Medical Association (JAMA), Vol. 302, Issue 18, 2009, p. 1970-1972.
-
Bakaimis B., Papanikolaou I. Electrical energy saving policies, initiatives, results, challenges and lessons learned for the Grevena hospital. Procedia Environmental Sciences, Vol. 38, 2017, p. 882-889.
-
Jiang C., Xing J., Ling J., Qin S. Energy consumption and carbon emissions of hospitals in Tianjin. Frontiers in Energy, Vol. 6, Issue 4, 2012, p. 427-435.
-
Blass A. P., Gouvea Da Costa S. E., Pinheiro De Lima E., Borges L. A. The measurement of environmental performance in hospitals: a systematic review of literature. Sustainable Operations Management, Springer, Cham, 2015, p. 75-102.
-
Sung W. P., Tzai-Tang T., Hsien-Jung W., MingJu W. Analysis of energy and carbon dioxide emission caused by power consumption. International Journal of Energy Research, Vol. 35, Issue 11, 2011, p. 1014-1022.
-
Gordillo Orquera R., Lopez Ramos L.-M., Muñoz Romero S., Iglesias Casarrubios P., Arcos Avilés D., Marques A. G., Rojo Álvarez J.-L. Analyzing and forecasting electrical load consumption in healthcare buildings. Energies Vol. 11, Issue 3, 2018, p. 493.
-
Wang T., Li X., Liao P.C, Fang D. Building energy efficiency for public hospitals and healthcare facilities in China: barriers and drivers. Energy, Vol. 103, 2016, p. 588-597.
-
Shi Y., Yan Z., Lv Z. An empirical study on the effect of energy saving measures against hospital energy consumption. DEStech Transactions on Engineering and Technology Research, 2019.
-
García Sanz Calcedo J., Al Kassir A., Yusaf T. Economic and environmental impact of energy saving in healthcare buildings. Applied Sciences, Vol. 8, Issue 3, 2018, p. 440.
-
Regulation (EC) No 1221/2009 of the European Parliament and of the Council of 25 November 2009 on the Voluntary Participation by Organizations in a Community Eco-Management and Audit Scheme (EMAS), Repealing Regulation (EC) No 761/2001 and Commission Decision 2001/681/EC, Bruxelles. European Parliament, 2009.
-
González A., García Sanz Calcedo J., Salgado D. R. A quantitative analysis of final energy consumption in hospitals in Spain. Sustainable Cities and Society, Vol. 36, 2018, p. 169-175.
-
Martinez De Salazar E., García Sanz Calcedo J. Study on the influence of maintenance operations on energy consumption and emissions in healthcare centres by fuzzy cognitive maps. Journal of Building Performance Simulation, Vol. 12, Issue 4, 2019, p. 420-432.
-
Axaopoulos J., Axaopoulos P., Gelegenis J., Fylladitakis E. D. Optimum external wall insulation thickness considering the annual CO2 emissions. Journal of Building Physics, Vol. 42, Issue 4, 2018, p. 527-544.
-
Romaní Picas J., Gracia Cuesta Cabeza A.-L.-F. Simulation and control of thermally activated building systems (TABS). Energy and Buildings, Vol. 127, 2016, p. 22-42.
-
Gao Z., Li Y., Ning Y. Survey and analysis of energy consumption of hospital buildings in Shandong Province. Proceedings Engineering, Vol. 205, 2017, p. 2485-2492.
-
Arango Miranda Hausler Romero Lopez Glaus R.-R.-R.-M., Ibarra Zavaleta S.-P. Carbon dioxide emissions, energy consumption and economic growth: a comparative empirical study of selected developed and developing countries. The Role of Exergy. Energies, Vol. 11, 10, p. 2018-2668.
-
Bonnema E., Pless S., Doebber I. Advanced energy design guide for small hospitals and healthcare facilities. Journal of Healthcare Engineering, Vol. 1, Issue 2, 2010, p. 277-296.
-
González A., García Sanz Calcedo J., Salgado D. R. Quantitative determination of potable cold water consumption in German hospitals. Sustainability, Vol. 10, Issue 4, 2018, p. 932.
-
Li Y. J., Yan Z. F. Study on analysis and share of energy consumption for large integral hospital buildings in the Chinese province of Shaanxi. Advanced Materials Research. Trans Tech Publications, 2012, p. 2817-2824.
-
Lopes M. A. R., Antunes C. H., Reis A., Martins N. Estimating energy savings from behaviours using building performance simulations. Building Research and Information, Vol. 45, Issue 3, 2017, p. 303-319.
Cited by
About this article

The authors wish to acknowledge the European Social Fund for the financial support provided through Research Projects GR18029 linked to the VI Regional Plan for Research, Technical Development and Innovation from the Regional Government of Extremadura (2017-2020). Also, the authors would like to express their thankfulness to the Ministerio de Ciencia, Innovación y Universidades (José Castillejo Program) for the financial assistance to Prof. Garcia-Sanz-Calcedo during the stay at University of Evora (Portugal), for the for the development of a part of this study.
