Abstract
The aim was to assess the cardiac function of healthy women by applying the spiritual intervention, i.e. a prayer, in different circumstances. Methods: a descriptive, intervention study design was used. The data were collected during three weeks in May, 2019. A total of 39 women with normal physiologic health at the age of 25-50 years who considered themselves as religious persons participated in the study. The cardiac-spiritual intervention process consisted of nine episodes with the heart rate measurements applied. For data recording and analysis researchers used ECG system Kaunas-Load that was developed at Lithuanian University of Health Sciences. With the ECG record RR interval, HRV and ST interval amplitude were analysed. The Spiritual Needs Questionnaire (SpNQ) was used to assess the spiritual needs of participants. Data were recorded and analyzed using the Statistical Package for Social Sciences (IBM SPSS Statistics) version 25.0. Results: Religious and Existential needs were the most important spiritual needs for women. Existential needs the most strongly correlated with Religious needs and needs of Inner peace. The reactions to prayer were more expressed in women of older age. The general tendency of increase in RR average during the praying episodes was observed; at resting position women’s heart rate decreased. During all phases of the study, the HR spectrum power was higher in the group of women with stronger expression of their unmet spiritual needs and the general physiologic condition of these women was also better. The increasing significant (p < 0.1) relationship between spiritual needs scores and changes of women heart rate was observed during pray episodes of spiritual intervention process. Conclusions: changes in the heart rate of healthy women during separate episodes of spiritual intervention demonstrated the reaction toward prayer. Individual or group praying caused the calming effect for women under the study. Assessment of unmet spiritual needs of women and the relationship with the heart rate changes during spiritual intervention process supported the idea that heart activity depends on the level of personal religiosity and spirituality.
Highlights
- The prayer, as healthy women’s individual or group interaction with higher power, causes the calming effect.
- The most important spiritual needs for healthy women are Religious and Existential needs.
- During spiritual intervention, higher HR spectrum power and better functional status of myocardium was in women with stronger expression of their spiritual needs.
1. Introduction
Population growth and ageing mean that the number of deaths from non-communicable causes increasing in most countries with cardiovascular disease as one of the leading causes of these deaths (17.9 million, 95 % UI 17.6 million to 18.3 million) in 2015. Ischemic heart disease and stroke accounted for 15·2 million deaths (15.0 million to 15.6 million) in 2015, equating to 85.1 % (84.7-85.5) of all deaths due to cardiovascular disease [1]. In Lithuania, 55.4 % of all deaths in 2018 were caused by circulatory system diseases [2].
Coping with the new circumstances for patients with chronic heart failure is challenging as their physical, psychological, social, cultural, and spiritual aspects are affected. Despite the recent advances in treatment of heart failure, most patients suffer debilitating and long-term symptoms putting increased demands on health systems [3].
Heart disease is a leading cause of death, but it's not inevitable. There are different strategies to protect the heart, to reduce the risk and to prevent heart disease: following a heart-healthy lifestyle, exercising, improving sleep and managing stress, having regular screenings. The heart function may be improved through spiritual interventions as well [4].
In recent years, spiritual well-being of a person and spiritual dimension of care have been investigated intensively. Spirituality is about the search for ultimate or transcendent meaning from different sources: religious practice, interpersonal relationship, connectedness with nature, music and the arts [5]. There is now substantial literature which demonstrates the positive effect of religious and spiritual beliefs on quality of life [6-8] and its indicators such as sleep quality and health status [9, 10], heart activity and heart failure-specific health status [11, 12]. Recent Lithuanian study determined the association of individually perceived importance of religiosity and spirituality with spiritual wellbeing and unmet spiritual needs [13].
There are different expressions of spirituality and various interventions may be applied in care practice (therapeutic intervention, deep communication, relaxation, yoga, meditation, prayer and others). On the other hand, review of Ross and Miles (2019) revealed that no single spiritual intervention was identified as effective in enhancing quality of life in patients with heart failure. Life review and relaxation/meditation didn’t prove any effect while conversations about spiritual matters, “spiritual coping” and a holistic person-centered team approach to care need further investigations [14].
For centuries, prayer has been used as an independent mean of feeling harmonious. Prayer, inherently a religious affair and activity, is distinguished as one of the forms of meditation, where one enters a state in which one feels inner harmony and higher connection with the environment. The prayer can be general or specific for oneself, for others or all; to a specific deity or may be offered more generally [15].
There are various discussions about the link between human spirituality and the physiologic state of the body. The changes in human organism that appear during prayer were not properly investigated and information about those changes is scarce.
The aim of our study was to assess the healthy women cardiac function by applying the spiritual intervention as a prayer in different circumstances.
2. Methods
2.1. Study design
A descriptive, intervention study design was used. The data were collected during three weeks in May, 2019. For data recording and analysis ECG system „Kaunas-Load” was used. The system was developed at Lithuanian University of Health Sciences (LUHS), Institute of Cardiology [16]. From ECG record RR interval (inter beat interval of the heart in [ms]), HRV (heart rate variability, total power – general activity of the heart autonomic nervous system) and ST interval amplitude (in [mkV] on 40-th [ms] after J point, reflecting efficacy of the heart hemodynamic) were analysed.
2.2. Participants and procedures
A total of 39 women participated in the study. The researchers applied to the faith communities looking for women volunteers to participate in the study. Women with normal physiologic health at the age of 25-50 years who considered themselves as religious persons were included in the convenient purposive sample.
Before intervention was started, participants were asked to fill in the questionnaire. They did it on their own. The Spiritual Needs Questionnaire (SpNQ) asks people to reflect on their unmet psychosocial, emotional, existential, and religious needs. According to this, the SpNQ differentiates four main factors: Religious Needs (6 items), Existential Needs (6 items), Needs for Inner Peace (4 items), Giving/Generativity and Forgiveness Needs (4 items). All items were scored with respect to the self-ascribed importance on a 4-point scale from disagreement to agreement (0 – not at all; 1 – somewhat; 2 – very; 3 – extremely) [17, 18]. The higher the scores, the stronger the respective needs are. To date, SpNQ was validated and used in Germany, Italy, Poland, Portugal, Brazil, Croatia, Iran, Philippines, Malaysia, China and Japan. The SpNQ-27 was translated and validated into Lithuanian by following the methodological considerations [19].
To determine the reliability, the internal consistency of the questionnaire was assessed. Internal consistency of the total SpNQ scale was very good (Table 1).
Table 1Internal consistency of Spiritual needs scale (SpNQ)
Subscales of SpNQ | No. of items | Cronbach α |
Religious needs | 6 | 0.788 |
Giving/generativity and Forgiveness needs | 4 | 0.918 |
Inner peace needs | 4 | 0.799 |
Existential needs | 6 | 0.790 |
Total scale | 27 | 0.931 |
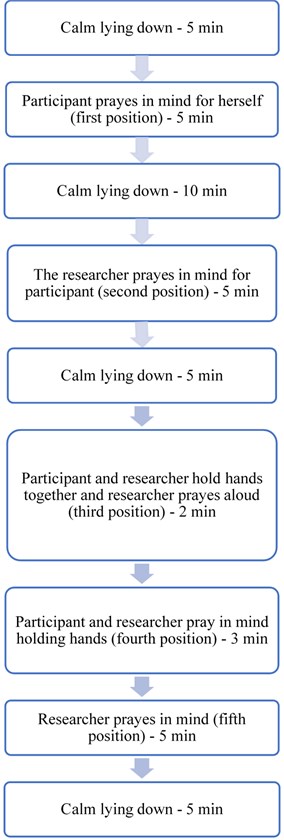
Fig. 1Intervention process
2.3. Cardiac-spiritual intervention
Women were asked their name as a code, year of birth, height and weight. The cardiac-spiritual intervention was applied that consisted of nine episodes (Fig. 1). The heart activity was registered by fastening the electrodes to patient's limbs and chest, for the registration of standard ECG.
At the beginning woman was rested in a comfortable lying position and electrodes placed. Next she was treated for 5 min. in calm, then for 5 min. she prayed in mind. Further she rested quietly for 10 min. Next 5 min the researcher says grace in mind for participant and then participant rests for 5 min. After researcher and participant holds hands for 2 min while researcher says grace vocally. Then researcher and participant continue to hold hands, and both pray in mind for 3 min. Further researcher continues with saying grace in mind for participant next 5 min. At the end the participant is lying down and resting quietly for 5min.
The grace that was said by participant and researcher:
God bless (name of the subject),
Let her thoughts be, God, Your thoughts, the thoughts of the good,
Let her works be done by her hands, O God
Let her works be seen by her eyes, O God
May her path lead you to God, and this path is full of peace, love, and self-realization
Let her discover more and more love, joy, and sharing with more people every day
Let it be surrounded only by good and loving people.
All in all, we pray to you God.
After recording the electrocardiogram, each woman was asked about her feelings and experience in the process of the intervention. Did she notice any unusual feelings in the body?
2.4. Statistical data analysis
Data were recorded and analyzed using the Statistical Package for Social Sciences (IBM SPSS Statistics) version 25.0. Descriptive statistics, single factor analysis of variance (One-Way ANOVA, with Bonferroni Post Hoc test comparing three or more groups), correlation (Spearman’s rho) were used to examine the data. Significance was defined by a p value of 0.05. Absolute values of correlation coefficient r < 0.20 was regarded as no or very weak correlation, between 0.20 and 0.29 as weak correlation, between 0.30 and 0.50 as moderate and > 0.5 as strong correlation. To assess psychometric properties of SpNQ scale, Cronbach’s alpha was calculated for internal consistency. Internal consistency that exceeded 0.6 was considered to be acceptable [20]. For the data analysis the women were divided in two groups according their age: younger age group, i.e. ≤ 38 years (56.4 %) and older age group, i.e. > 38 years (43.6 %).
2.5. Ethical considerations
The Lithuanian Regional Committee on Bioethics issued the permission to conduct the study (29 April, 2019, No. BEC-IL(B)-221). Participants received written and oral information about the aim of the study and gave their informed consent for participation and observations. Data confidentiality was guaranteed by no identifying information being recorded on answers.
3. Results
There were all females in the sample (N-39). The age of participants ranged from 21 to 55 years. The mean age was 37.3±10.9. All women were considered themselves as believers in God.
3.1. Assessment of the spiritual needs
Assessment of the spiritual needs revealed that the most important needs for women were Religious and Existential needs, while Giving/Generativity and Forgiveness needs and Inner peace needs were scored lower, but nevertheless high (Table 2).
Table 2Mean scores of four spiritual needs domains.
Needs | Mean score ±SD | Median | Minimum | Maximum | Percentiles | ||
25 | 50 | 75 | |||||
Religious | 16.0±2.6 | 18.0 | 9.0 | 18.0 | 14 | 18 | 18 |
Giving/Generativity and Forgiveness | 11.1±1.6 | 12.0 | 5.0 | 12.0 | 11 | 12 | 12 |
Inner peace | 9.2±2.6 | 9.0 | 4.0 | 12.0 | 7 | 9 | 12 |
Existential | 14.8±3.6 | 17.0 | 5.0 | 18.0 | 12 | 17 | 18 |
Correlation analysis revealed strong and moderate positive associations among each of four SpNQ domains. Existential needs correlated with the Religious needs and needs of Inner peace the most strongly (Table 3).
Table 4Inter-correlation of spiritual needs
Variables | Religious needs | Giving/generativity and Forgiveness needs | Inner peace needs | Existential needs |
Religious needs | 1.000 | 0.488** | 0.727** | 0.872** |
Giving/generativity and Forgiveness needs | 1.000 | 0.481** | 0.436** | |
Inner peace needs | 1.000 | 0.833** | ||
Existential needs | 1.000 | |||
**Correlation is significant at the 0.01 level (2-tailed) | ||||
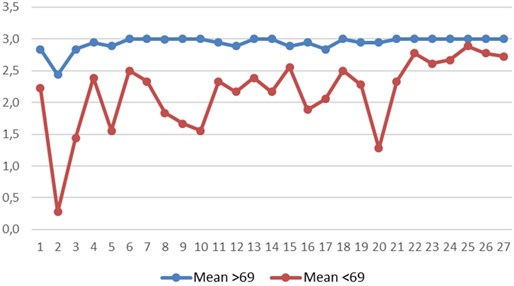
In the analysis the mean value of all 27 items of SpNQ ratings was calculated and the women were divided into two groups: those with the mean value of < 69 (18.5 %) and with the mean value of > 69 (21.5 %).
Fig. 2SpNQ item ratings in two groups of women. Y axis – mean of answers to each SpNQ item; a mean of all answers: more than 69 (blue curve) and less than 69 (red curve); X axis – SpNQ item number.
After the study women were asked at which time of the intervention, if any, they did feel unusual. According to women’s statements they were divided into two groups. The first group (N = 28, 72 %) did not have unusual feelings or have had very slight sensation, and the second group (N = 11, 28 %) have had a clear sense of connection (i.e. pleasant relaxation, uplifting feeling). The cardiogram records of women with exceptional feelings were analyzed and then compared with the first group of women without any specific feelings.
3.2. Changes of women cardiac function in relation to prayer
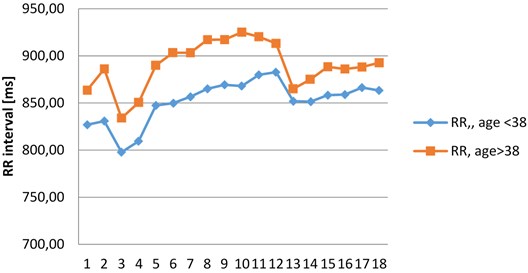
In older women group (> 38 y. and the mean age – 46.7±7.65 y.) RR interval was more expanded (i.e. slower heart rate) than in the younger women group (< 38 y. and mean age – 29.0±5.47 y.), although the reactions to prayer were more expressed in women of older age (Fig. 3).
Fig. 3RR interval changes in two age groups of women
Similar reactions of heart rate (HR) to prayer were observed in both age groups of women during different episodes of spiritual intervention process (Fig. 4).
Fig. 4RR interval changes in two age groups of women during different episodes of spiritual intervention process
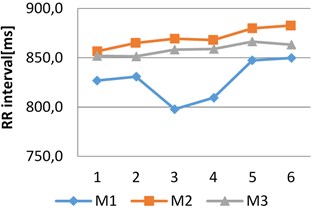
a) RR changes during M1, M2, M3, age <38
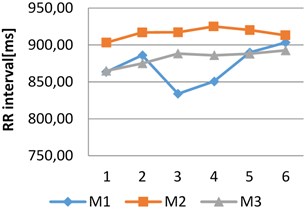
b) RR changes during M1, M2, M3, age >38
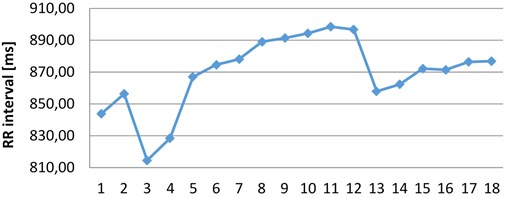
During the spiritual intervention process, the average changes of RR interval were assessed. The general tendency of increase in RR average during the praying episodes was determined. At the resting position women’s heart rate decreased (1;2 and 5;6 episodes) (Fig. 5).
The most clearly expressed increase in the heart rate was observed during the 1st and 3rd episode of praying (at 12 and 13 episode of praying HR increases and at 14 and 15 episode of praying HR decreases in Fig. 5). These results prove that praying, as individual or group interaction with higher power, causes the calming effect for women under the study (Fig. 5).
Fig. 5RR interval changes during the different measurement episodes of spiritual intervention process
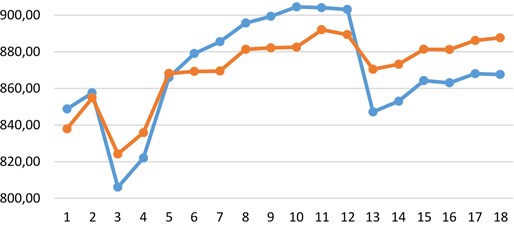
In relation to the SpNQ scores, women were divided into two groups: those who rated their unmet spiritual needs with a summative mean score of 69 and more and those who rated with less score than 69. The higher mean score reflects higher importance of psychosocial, emotional, existential, and religious needs for women under the study. Fig. 6 demonstrates that the most expressed heart rate reactions of women toward praying were in the group with the average ratings over 69.
Fig. 6Reactions toward praying in relation to different level of unmet spiritual needs of women (blue – Quest > 69; red – Quest < 69)
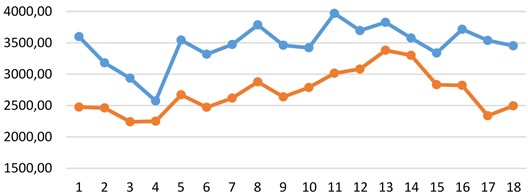
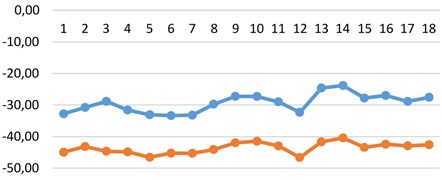
Similarly, the general power (general activity of the heart autonomic nervous system) of HR spectrum differs in both spiritual needs groups. During all episodes of intervention process, the HR spectrum power was higher in the group of women with stronger expression of their unmet spiritual needs (mean > 69). The general physiologic condition of these women was also better. Initial HR measures in relation to women age did not have any significant differences in both age groups (Fig. 7).
Fig. 7HR spectrum power (general autonomic activity) in relation to the different importance of women’s unmet spiritual needs (blue – Quest > 69; red – Quest < 69)
Further the changes in ST amplitude were analysed. The results were consistent with the findings on HRV spectrum power differences in both groups of women in relation to the importance of women’s unmet spiritual needs. Clinical interpretations of this measure reflect the hemodynamic efficacy of heart myocardium: in the group of women with stronger expression of their spiritual needs functional status of myocardium was better (Fig. 8).
Fig. 8ST amplitude in relation to the different importance of women’s unmet spiritual needs (blue – Quest > 69; red – Quest < 69)
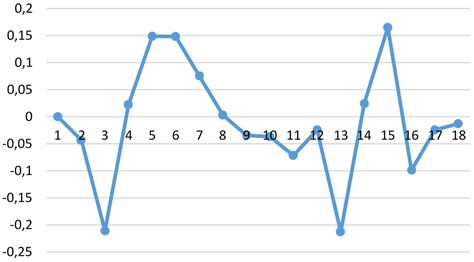
Correlation analysis of spiritual needs scores and changes of the heart rate during the episodes of spiritual intervention revealed increasing significant (p < 0.1) relationship of these two variables during the 1st and 3rd episode of praying process (Fig. 9).
Fig. 9Correlation analysis Corr(Quest; Dif(RRi+1 – RRi)) of spiritual needs scores and changes of the heart rate during the episodes of spiritual intervention process
4. Discussion
The most important spiritual needs for women under this study were Religious needs and that is consistent with the fact that all participants consider themselves as religious persons and agreed to participate in spiritual intervention testing. The Giving/Generativity and Forgiveness needs and Inner peace needs were scored at the lowest level possibly because the participants were healthy women of the young or middle age.
As in previous study [21], interconnection among each of four SpNQ domains was strongly or moderately positive showing that spiritual needs are the one whole phenomenon with four different but highly interconnected domains.
Correlation analysis of spiritual needs scores and changes of the heart rate of women during various phases of spiritual intervention shows that reaction toward prayer depends on their personal religiosity and spirituality level that was reflected by the standardized assessment of unmet spiritual needs (i.e. SpNQ survey). The results support the idea that women by being in a higher need of spiritual connectedness and support demonstrate stronger reaction toward prayer and better physiologic functioning.
During the spiritual intervention process in this study, the general tendency of increase in RR average during the praying episodes was observed although at the resting position heart rate of women decreased. When a person is in a more coherent state there is a shift in the relative autonomic balance toward increased parasympathetic activity (vagal tone), increased heart-brain synchronization and entrainment between diverse physiologic systems. In this mode, the function of body systems with a high degree of efficiency, harmony and natural regenerative processes is facilitated. Although physiologic coherence is a natural human state that can occur spontaneously, sustained episodes generally are rare. While some rhythmic-breathing methods may induce coherence for brief periods, our research indicates that people can achieve extended periods of physiologic coherence by actively self-generating positive emotions. When functioning in a coherent mode, the heart pulls other biologic oscillators into synchronization with its rhythms, thus leading to entrainment of these systems.
Our study revealed that during all episodes of spiritual intervention process the HR spectrum power was higher in the group of women with stronger expression of their unmet spiritual needs (mean >69) and the general physiologic condition of these women was also better. Changes of HR during sessions of praying show the changes in regulatory system of human organism, and that is quite explainable, having in mind psychologic effect of praying. Interesting from our point of view, that it was reflecting in heart metabolic features as well, i.e. in ST amplitude. It shows, that spirituality and physiology are strongly connected features of human organism. It could be postulated that when such coherence inside the human organism is achieved, it could be in higher interconnection with outer world. Many articles to support this idea was published by Rollin McCraty (2015; 2018) [22, 23].
Results of this study essentially underscore what people have intuitively known: positive emotions stimulate humans not only “to feel better”, they actually tend to increase synchronization of the body systems, thereby enhancing energy and enabling us to function with greater efficiency and effectiveness, and create a higher coherence with surrounding. When we observe higher positive interconnection in a group of people then higher “heart-to-heart synchronization across subjects could be found, lending credence to the possibility of heart-to-heart bio-communications” [24]. And such effects are not depending on the kind of religion [25].
5. Conclusions
Changes of the heart rate of healthy women during separate episodes of spiritual intervention demonstrated the reaction toward praying. Assessment of unmet spiritual needs of women and the relationship of these needs with the heart rate changes during spiritual intervention process supported the idea that cardiac function depends on the level of personal religiosity and spirituality. Women by being in a higher need of spiritual connectedness and support demonstrate stronger reaction toward praying and have better physiologic functioning.
References
-
GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study. Lancet, Vol. 388, Issue 10053, 2016, p. 1459-1544, https://doi.org/10.1016/S0140-6736(16)31012-1.
-
Health Information Centre of Institute of Hygiene. Causes of death, 2019 (provisional data). http://www.hi.lt/index.php?mact=News,cntnt01,detail,0&cntnt01articleid=1469&cntnt01returnid=503.
-
Ponikowski P., van Veldhuisen D. J., Comin-Colet J., et al. Beneficial effects of long-term intravenous iron therapy with ferric carboxymaltose in patients with symptomatic heart failure and iron deficiency. European Heart Journal, Vol. 36, Issue 11, 2015, p. 657-668.
-
Mangolian Shahrbabaki P., Nouhi E., Kazemi M., Ahmadi F. Spirituality: A panacea for patients coping with heart failure. International Journal of Community Based Nursing and Midwifery, Vol. 4, Issue 1, 2017, p. 38-48.
-
Astrow A. B., Puchalski C. M., Sulmasy D. P. Religion, spirituality, and health are: social, ethical, and practical considerations. American Journal of Medicine, Vol. 110, Issue 4, 2001, p. 283-287, https://doi.org/10.1016/s0002-9343(00)00708-7.
-
Unterrainer H. F., Lukanz M., Pilch M., Scharf S., Glawischnig-Goschnik M., Wutte N., Fink-Puches R., Aberer E. The influence of religious/spiritual wellbeing on quality of life in dermatological disease. British Journal of Dermatology, Vol. 174, Issue 6, 2016, p. 1380-1383, https://doi.org/10.1111/bjd.14359.
-
Pilger C., Santos R., Lentsck M. H., Marques S., Kusumota L. Spiritual wellbeing and quality of life of older adults in hemodialysis. Revista Brasileira de Enfermagem, Vol. 70, Issue 4, 2017, p. 689-696, https://doi.org/10.1590/0034-7167-2017-0006
-
Bai M., Lazenby M. A systematic review of associations between spiritual wellbeing and quality of life at the scale and factor levels in studies among patients with cancer. Journal of Palliative Medicine Vol. 18, Issue 3, 2015, p. 286-298, d https://doi.org/oi: 10.1089/jpm.2014.0189
-
Eslami A. A., Rabiei L., Khayri F., Rashidi Nooshabadi M. R., Masoudi R. Sleep quality and spiritual wellbeing in hemodialysis patients. Iranian Red Crescent Medical Journal, Vol. 16, Issue 7, 2014, p. e17155. https://doi.org/10.5812/ircmj.17155.
-
Phillips K. D., Mock K. S., Bopp C. M., Dudgeon W. A., Hand G. A. Spiritual wellbeing, sleep disturbance, and mental and physical health status in HIV-infected individuals. Issues in Mental Health Nursing, Vol. 27, Issue 2, 2006, p. 125-139, https://doi.org/10.1080/01612840500436917.
-
Mashhadimalek M., Jafarnia Dabanloo N., Gharibzadeh S. Is it possible to determine the level of spiritual wellbeing by measuring heart rate variability during the reading of heavenly books? Applied Psychophysiology and Biofeedback Vol. 44, Issue 3, 2019, p. 185-193, https://doi.org/10.1007/s10484-019-09433-3
-
Flint K. M., Fairclough D. L., Spertus J. A., Bekelman D. B. Does heart failure-specific health status identify patients with bothersome symptoms, depression, anxiety and/or poorer spiritual wellbeing? European Heart Journal – Quality of Care and Clinical Outcomes, Vol. 5, Issue 3, 2019, p. 233-241, https://doi.org/10.1093/ehjqcco/qcy061.
-
Riklikiene O., Spirgiene L., Kaseliene S. Association of religiosity and spirituality with the perception of cancer patients’ spiritual wellbeing and spiritual needs. Nursing Education, Research, and Practice, Vol. 9, Issue 1, 2019, p. 19-26.
-
Ross L., Miles J. Spirituality in heart failure: a review of the literature from 2014 to 2019 to identify spiritual care needs and spiritual interventions. Current Opinion in Supportive and Palliative Care, 2019, https://doi.org/10.1097/SPC.0000000000000475.
-
Sharma S., Sharma M. Sustaining and enhancing health/well-being of Indian students: The role of certain spiritual and religious interventions. Psychological Studies, Vol. 51, Issue 2, 2006, p. 113-118.
-
Zumbakyte-Sermuksniene R., Kajeniene A., Vainoras A., Berskiene K., Augutiene V. Assessment of functional conditions of basketball and football players during the load by applying the model of integrated evaluation. Medicina, Kaunas, Vol. 46, Issue 6, 2010, p. 421-428, https://doi.org/10.3390/medicina46060059.
-
Büssing A., Recchia D. R., Koenig H., Baumann K., Frick E. Factor structure of the spiritual needs questionnaire (SpNQ) in persons with chronic diseases, elderly and healthy individuals. Religions, Vol. 9, Issue 1, 2018, p. 1-11, https://doi.org/https://doi.org/10.3390/rel9010013
-
Büssing A., Balzat H.-J., Heusser P. Spiritual needs of patients with chronic pain diseases and cancer – validation of the spiritual need’s questionnaire. European Journal of Medical Research, Vol. 15, 2010, p. 266-273, https://doi.org/10.1186/2047-783X-15-6-266
-
Riklikienė O., Spirgienė L., Kaselienė S., Luneckaitė Ž., Tomkevičiūtė J., Büssing A. Translation, cultural, and clinical validation of the Lithuanian version of the spiritual needs questionnaire among hospitalized cancer patients. Medicina, Kaunas, Vol. 55, Issue 11, 2019, p. E738, https://doi.org/10.3390/medicina55110738.
-
Bland J. M., Douglas G. A. Statistics notes: Cronbach’s alpha. British Medical Journal, Vol. 314, Issue 7080, 1997, p. 572.
-
Riklikiene O., Tomkeviciute J., Spirgiene L., Valiuliene Z., Büssing A. Spiritual needs and their association with indicators of quality of life among non-terminally ill cancer patients: cross-sectional survey. European Journal of Oncology Nursing. Vol. 44, 2019, p. 101681, https://doi.org/10.1016/j.ejon.2019.101681
-
Mccraty R., Atkinson M., Timofejeva I., Roza Joffe R., Vainoras A., Landauskas M., Alabdulgader A. A., Ragulskis M. The influence of heart coherence on synchronization between human heart rate variability and geomagnetic activity. Journal of Complexity in Health Sciences, Vol. 1, Issue 2, 2018, p. 42-48, https://doi.org/10.21595/chs.2018.20480
-
McCraty R., Shaffer F. Heart rate variability: new perspectives on physiological mechanisms, assessment of self-regulatory capacity, and health risk. Global Advances in Health and Medicine, Vol. 4, Issue 1, 2015, p. 46-61.
-
Morris S. M. Facilitating collective coherence: group effects on heart rate variability coherence and heart rhythm synchronization. Alternative Therapies in Health and Medicine, Vol. 16, Issue 4, 2010, p. 62-72.
-
Sarwari A. Q., Abdul Wahab M. N. The relationship between Zikr (Remembrance of Allah), heart coherence and intrapersonal communication among Muslim postgraduate students from different countries. Journal of Language and Communication, Vol. 5, Issue 1, 2018, p. 110-123.
About this article

